Proctological pathology
Hemorrhoid during pregnancy
 Print this article
Print this article Download the article
Download the article Making an appointment
Making an appointmentPathology
What is a hemorrhoid (pile)?
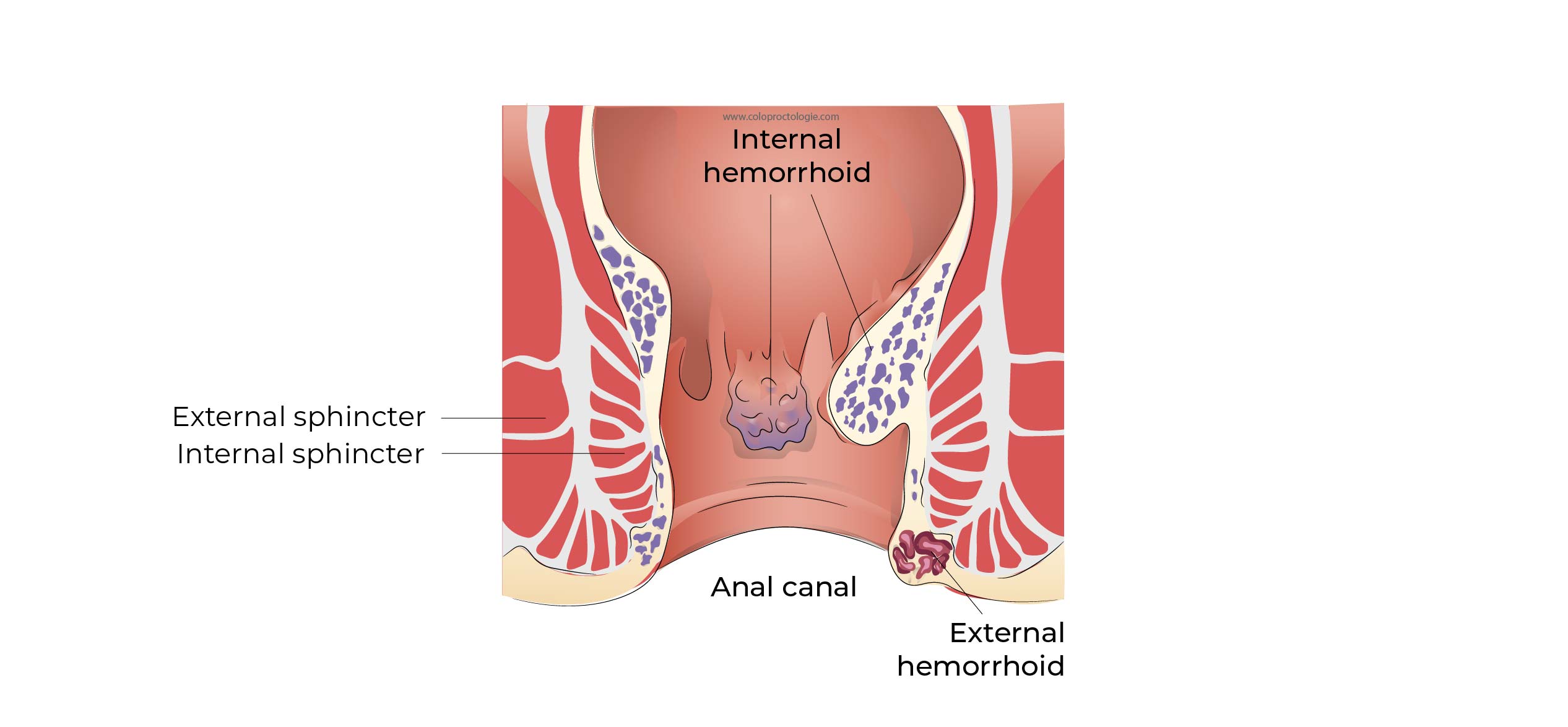
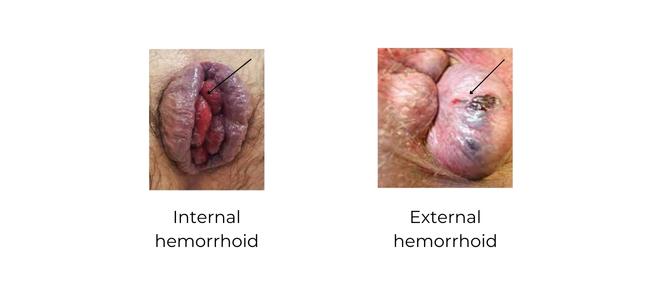
A hemorrhoid is a bundle of vascular tissue consisting of a network of small veins and small arteries located in the anal canal. Hemorrhoids are present in the anal canal in every person at birth.
The presence of a hemorrhoid is not a disease.
Normally, a hemorrhoid is not painful.
What is the function of hemorrhoids (pile)?
The function of hemorrhoids is not fully understood. It helps in continence issues. With age, the muscles of the pelvic floor weaken, as does the anal sphincter. When the muscles weaken, the hemorrhoids help to seal off the anal canal and help to keep the continence.
Over time in geriatric patients, the contribution of hemorrhoids to continence can reach 15-20%.
When do we speak of hemorrhoidal disease?
It is called a disease or pathology when hemorrhoids become symptomatic:
– Bleeding
– Anal pain
– Urge to defecate (pressing sensation in the anus)
– Hemorrhoids appear outside the anal canal (prolaps).
What are the symptoms of hemorrhoids (pile)?
Bleeding
Bright red, non-painful bleeding, especially after bowel movements. Blood may be visible in the toilet bowl or on the toilet paper.
Depending on the patients, additional tests may be prescribed to rule out inflammatory bowel disease or colorectal cancer.
- If the bleeding is mixed with the stools (black stools).
- Blood loss is accompanied by a change in the frequency and consistency of stools. Blood loss is accompanied by abdominal pain
- If over 40 years of age
- If chronic blood loss
Anal pain
- Due to thrombosis of an external or mixed hemorrhoid.
Prolaps
-
Exteriorization of hemorrhoids outside the anal canal due to squeezing during defecation.
Tenesmus: (false urge, feeling of wanting to defecate)
- Due to swelling of the hemorrhoids in the anal canal, the patient feels pressure in the anal canal and may have a false urge to defecate.
Anal pruritus / irritation / mild incontinence
- The presence of hemorrhoids in the anal canal can prevent complete sealing of the anal canal, leading to fluid loss, irritation and mild incontinence.
Are hemorrhoids (pile) common during pregnancy and after childbirth?
- Complaints of hemorrhoids affect 25-30% of pregnant women. After delivery, 20% of women suffer from thrombosis of external hemorrhoids and 7.8% in the last trimester of pregnancy.
- Risk of thrombosis after caesarean section: 4%.
- Risk of thrombosis after vaginal delivery +/- 20%.
Why do hemorrhoids occur more frequently during pregnancy and after childbirth?
- Foetal pressure in the abdominal cavity increases the resistance of venous blood flow. The increased pressure in the abdomen makes it harder for blood to flow back to the heart. Venous and lymphatic blood can accumulate in the legs and also in the hemorrhoids.
- The constipation during pregnancy, necessitates harder and more frequent pressing during defecation which can lead to prolapsing of the hemorrhoids (hemorrhoids pushed outside the anal canal).
- Pressing during labour itself can also cause hemorrhoidal prolapse.
Hormonal changes during pregnancy and hormonal changes after childbirth affect the hemorrhoidal tissue. Under the influence of these hormonal fluctuations, the supporting tissue of the hemorrhoids becomes looser.
Factors contributing to hemorrhoidal symptoms:
– Childbirth after 39.7 weeks
– A large baby
– A long first stage of labour
Rouillon JM. Analyse de l’incidence et des facteurs éthiopathogéniques des thromboses hémorroïdaires du post partum Gastroenterol Clin Biol 1991; 15 : A300.
Abramowitz L. Anal fissure and thromboses external hemorroids before and after delivery. Dis Colon Rectum 2002; May; 45 (5): 650- )
Thompson JF, Roberts CL, Currie M, Ellwood DA. Prevalence and persistence of health problems after childbirth : associations with parity and method of birth. Birth. 2002 Jun;29(2):83-94.
Treatment
Treatment of hemorrhoids during pregnancy and postpartum?
Conservative treatment (non-surgical) of hemorrhoids is the treatment of choice. Two-thirds of patients will have no more symptoms of hemorrhoids 6 months after delivery.
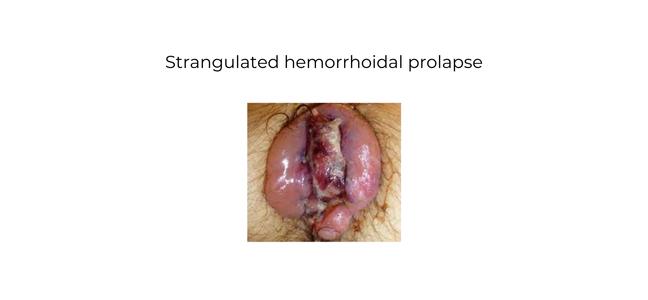
Patients may have strangulated internal hemorrhoids or thrombosed external hemorrhoids.
In most patients, the pain regresses after 2 to 4 days with conservative treatment (non-surgical).
If the pain persists despite maximum conservative treatment, surgical intervention may be considered to relieve the pain. If necrosis of the hemorrhoids occurs, an urgent surgical intervention may be necessary.
Thompson JF, Roberts CL, Currie M, Ellwood DA. Prevalence and persistence of health problems after childbirth : associations with parity and method of birth. Birth. 2002 Jun;29(2):83-94.
Conservative treatment
- High-fibre diet and hydration.
- Laxative for constipation.
- Avoid prolonged standing position as it increases pressure in the hemorrhoids. Semi-recumbent position in sofa or armchair.
- If you have to sit for a long time: try sitting on a cushion to relieve pressure, walk around for a few minutes every hour.
- Sitting bath: 5 -10 min at +/- 40°C to relieve pain.
- Ice pack: 10min to 4x/day to reduce swelling
- Analgesic ointment (Xylocaine gel 5%)
- Hemorrhoid ointment: Sheriproct, Cosanal, Trianal, …
- Flavonoid (Daflon venotonic)
- Rutin Trihydrate, Solgar Rutin 500mg 2x /d, Rutoside 2x /d
- Pain relief:
– Dafalgan forte 1gr 3-4x /day
– Morphine Tradonal if needed
Surgical treatment
Surgical treatment includes excision of one or more of the painful hemorrhoids.
See surgical procedure: hemorrhoid (pile) resection /hemorrhoidectomy
Analgesics during pregnancy and lactation
Pregnancy
It is recommended not to use analgesics during pregnancy that are not approved or prescribed by a doctor: self-medication is strongly discouraged.
Non-opioid analgesics (level 1)
Paracetamol is preferred regardless of the duration of pregnancy.
Before 24 weeks: Aspirin and NSAIDs can be used intermittently during the first five months of pregnancy (24 weeks of amenorrhoea).
Chronic use should be avoided during this period if possible.
After 24 weeks: Aspirin ≥500 mg/d and NSAIDs are contraindicated until delivery.
Weak opioid analgesics (level 2)
Codeine or tramadol may be used regardless of gestational age.
Mixed or strong opioid analgesics (level 3)
Morphine is preferred regardless of the duration of pregnancy.
Breastfeeding
Depends on the nature and intensity of the pain:
Among drugs, a level 1 analgesic or a corticoid should be recommended as first choice if possible, before moving on to a level 2 or 3 analgesic (painkiller).
Non-opioid analgesics and NSAIDs (level 1)
Any of the following drugs may be chosen during breastfeeding:
– Paracetamol
– Ibuprofen
– Ketoprofen
– Flurbiprofen
– Diclofenac
– Celecoxib
– Aspirin as a single dose
Weak opioid analgesics (stage 2), if stage 1 is not appropriate (see above)
Tramadol
In the first 4 days after delivery, oral tramadol may be used when breastfeeding.
After this period, treatment with tramadol during breastfeeding may be considered if it is of short duration ( 2 to 3 days) and in the lowest possible dose.
Codeine
In the first 2 weeks after childbirth, it is better not to use codeine.
After the first 2 weeks, treatment with codeine may be considered, provided it is of short duration (2 to 3 days) and in the lowest possible dosage. In case of poor maternal tolerance (sedation, nausea, etc.), codeine should be reduced or even stopped.
Mixed or strong opioid analgesics (level 3)
Within 3 days of delivery:
Nalbuphine or morphine can be used.
If treatment with a level 3 analgesic is necessary after 3 days, breastfeeding should be suspended.