Proctological pathology
Anal fissure
 Print this article
Print this article Download the article
Download the article Making an appointment
Making an appointmentPathology
What is an anal fissure?
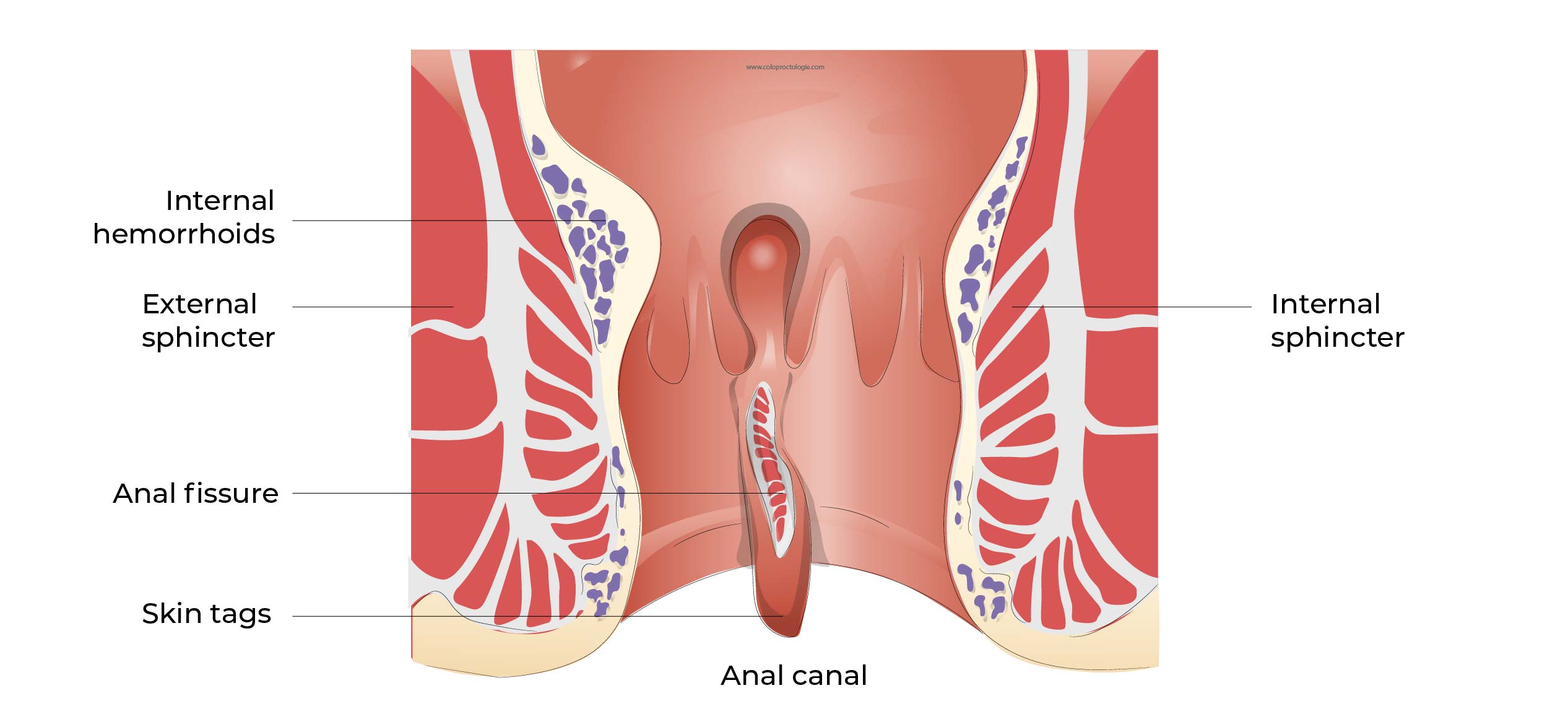
- An anal fissure is a superficial tear (a wound) on the inner layer (mucosa/mucosa) of the anal canal. The fissure is often not visible from the outside.
- Average age 39 years.
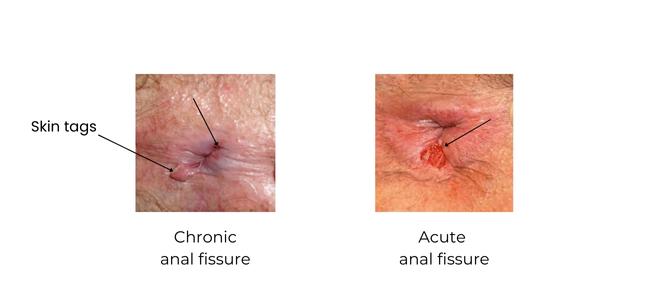
Type of anal fissure:
– Acute anal fissure: present for less than 4 weeks.
– Chronic anal fissure: recurrent fissure or fissure present for more than 4 weeks.
What are the symptoms of an anal fissure?
- Anal pain (90.8%) during defecation that can last up to 2-3 hours. As a result the patient has anxiety about going to the toilet and defecating. The patient tends to postpone defecation, thus worsening the constipation which increases the pain during defecation.
- Burning sensation after defecation.
- Blood loss (71.4%) after defecation on toilet paper.
(Hanalel et al Dis Colon Rectum 1997; 40 (2):229-233)
All 3 symptoms may occur with varying frequency and intensity.
The symptoms are intensified with hard stools and during periods of constipation.
Sometimes an abscess may form behind the fissure (retro-fissural abscess). The patient may then complain of a foul smelling discharge.
Why do you suffer from an anal fissure?
The origin of anal fissure is not always known.
In most cases, anal fissure occurs as a result of trauma to the mucosa (surface layer) of the anal canal.
As a result of the pain, the muscle of the anus (sphincter) contracts (spasm). This increases the pain and reduces the blood supply to the wound, preventing the fissure from healing.
As a result of the pain, a vicious cycle develops, the patient delays defecation, the stool stays longer in the colon and becomes harder because more water is withdrawn from the stool in the colon… The harder stool (constipation) again hurts the anal fissure preventing it from healing and increases the pain during defecation.
Trauma:
– Constipation
– Traumatic perineal hygiene (traumatic rubbing with toilet paper)
– Sexual practices (sodomy, foreign body)
In a minority of cases, the origin may be due to an inflammatory disease of the colon such as Crohn’s disease, a sexually transmitted disease or a tumor of the anal canal.
How is an anal fissure diagnosed?
The diagnosis is made based on the history (conversation with the patient) and the proctological examination.
Outspoken pain in the anal canal at palpation or even at rest. Sometimes inspection of the perineum is sufficient. An endoscopic examination is rarely performed. If the fissure is present for a long time, a swelling of the mucosa at the edge of the fissure may be visible, which may be mistaken for an haemorrhoid
(piles).
Most fissures are located on the posterior part of the anal sphincter and, to a lesser extent, on the anterior part.
If the location of the fissure is different or if there are multiple fissures, other causes of anal fissures should be considered. (Crohn’s, sexually transmitted diseases, tumors…)

Is an anal fissure dangerous?
An anal fissure does not increase the risk of cancer.
An ulcer (wound) in the anal canal that persists despite treatment should be examined and, if necessary a biopsy should be performed to rule out malignancy.
A fissure with an atypical location can suspicious and may require further investigation.
If bleeding is part of the symptoms, depending on the age (over 50 years) or family history, a colonoscopy will be requested after the anal fissure has healed.
What can I do to prevent anal fissure?
-
Preventing constipation
Not holding stools, the longer stools stay in the rectum and colon the more reabsorption of water from the stool and thus harder stools.
Not holding stools while traveling (plane, train, workplace…)
- High-fibre diet and adequate hydration (1.5-2 l per day).
- If necessary, use mild laxatives such as Lansoyl®.
- Physical exercise to stimulate transition.
- Avoid aggressive anal hygiene (do not rub to hard): soft toilet paper.
Treatment
What are the possible conservative treatments?
In most cases, anal fissure can be treated without surgery.
Treatment involves changing the consistency of stools, reducing constipation or diarrhea, reducing pain and promoting blood circulation in the wound to break the vicious cycle.
Looser stools
- High-fibre diet and adequate hydration: 1.5-2l.
- Fibre supplements in the diet. Treatment with cream to be applied 2x/day in the anal canal.
Laxatives
- Paraffin (Lansoyl® 3x/day: one spoonful 15 min before meals)
- If necessary macrogol (Movicol®) sachets 2-3x/day
- Physical exercises to stimulate the bowel transit.
Treatment of pain
- 10-20 minutes warm baths, reduces pain and relaxes the anal sphincter.
- Analgesic:
– Paracetamol 1gr 3-4x/day. (Dafalgan®…)
– Non-steroidal anti-inflammatory drugs (Brufen® 400mg 3x/jr, Cataflam®, Voltaren®, Diclofenac®…)
– Morphinique if needed (Tradonal Odis 50mg…)
Cream/ointment
→ Xylocaïne 5% gel:
– Anaesthetic ointment to be applied in the anal canal (on and around the fissure).
–Apply 3-4x/day
→ Diltiazem and Isosorbide dinitrate based local ointment:
Exemples: Rectogesic®, magistral preparation…
– Applying the ointment relaxes tension in the sphincter of the anal canal. This improves blood flow to the anal fissure and thus healing.
– The cream should be applied in the anal canal 2-4 times a day. The cream should be applied to the anal muscle (this can be done with a condom or with a cut finger from a plastic glove).
– Treatment usually lasts 4 weeks. If symptoms subside quickly, the frequency and duration of application of the cream can be reduced after consultation with your doctor.
– Healing of the fissure: 40-60%.
– Side effect of the ointment: Headache: 15-39%
Cochrane library ; Review. Operative procedures in fissura in ano ; Nov 2011
Richard Nelson British medical journal Clinical Evidence 2014;11:407
JH ScholefieldA dose finding study with 0.1%, 0.2%, and 0.4% glyceryl trinitrate ointment in patients with chronic anal fissures Gut 2003 52 (2) 264-269
A Comparison of Injections of Botulinum Toxin and Topical Nitroglycerin Ointment for. the Treatment of Chronic Anal Fissure N Engl J Med 1999; 341:65-69
What are the possible surgical treatments?
The surgery (that will be recommended,) is determined on a case-by-case basis, according to the characteristics of the anal fissure and the patient.
- Fissurectomy and injection of Botulinum toxin ( Botox®)
Surgery involves excision of the fissure to allow the wound to heal. Botulinum toxin is injected into the internal sphincter, causing a partially and temporarily paralysis of the muscle. The tension of the anal sphincter decreases and the blood supply to the wound increases. The increase in blood supply promotes the wound healing.
See surgical procedure: Fissurectomy and injection of Botulinum toxin (Botox®)
- Fissurectomy and lateral sphincterotomy
Surgery involves excision of the fissure to allow the wound to heal.. The internal sphincter is partially incised to reduce the tension of the anal sphincter. And thus the blood supply of the wound increases and healing of the wound is promoted).
See surgical procedure: Fissurectomy and lateral sphincterotomy
- Fissurectomy and anoplasty
The surgery consists of excising the fissure and covering the wound with healthy tissue.