Colorectal pathology
Acute diverticulitis
 Print this article
Print this article Download the article
Download the article Making an appointment
Making an appointmentPathology
What is a diverticulum – diverticulosis – diverticulitis of the colon?
Diverticulum:
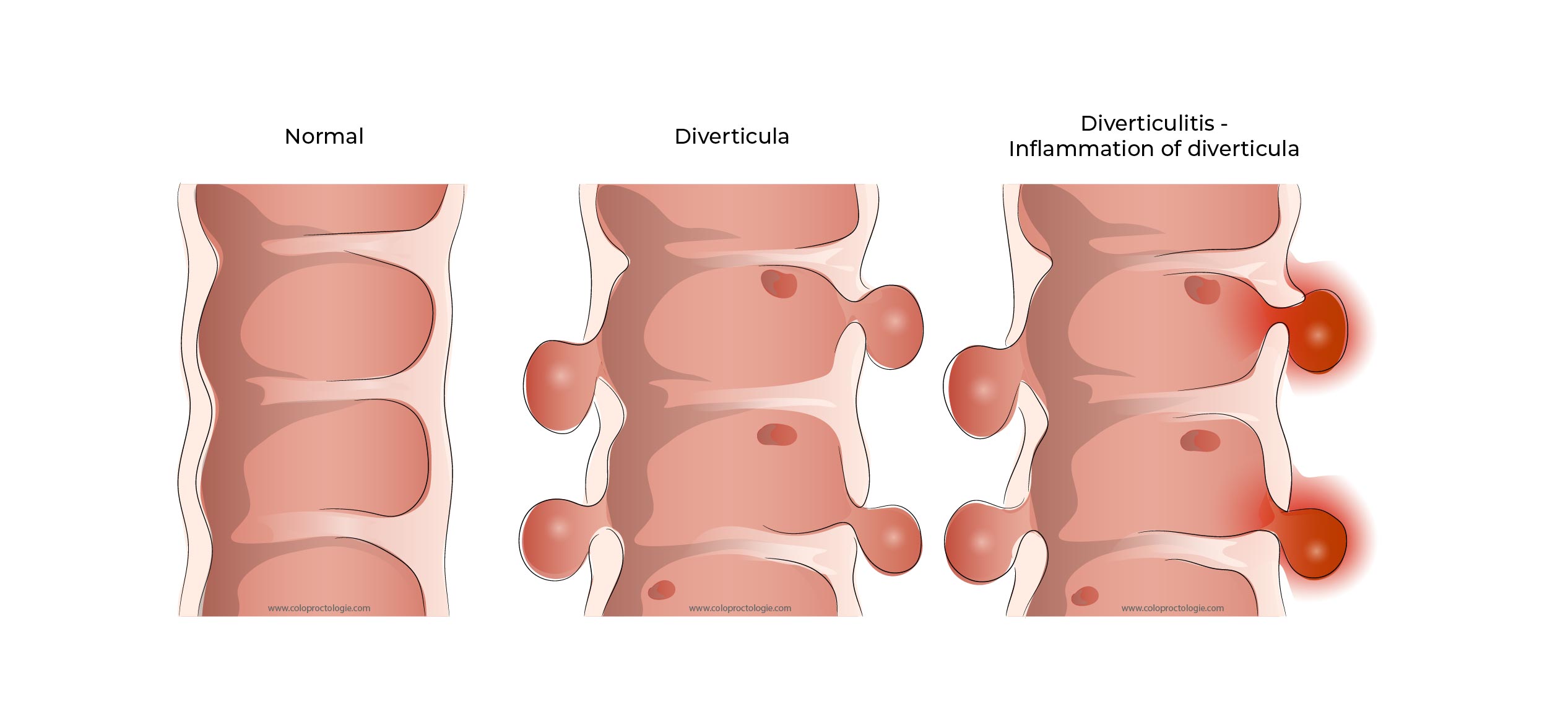
The wall of the colon consists of several layers. The innermost layer is the mucous layer (mucosa) followed by the submucosal layer, then the muscular layer (the thickest part of the colon) and finally the fine serosa on the outside.
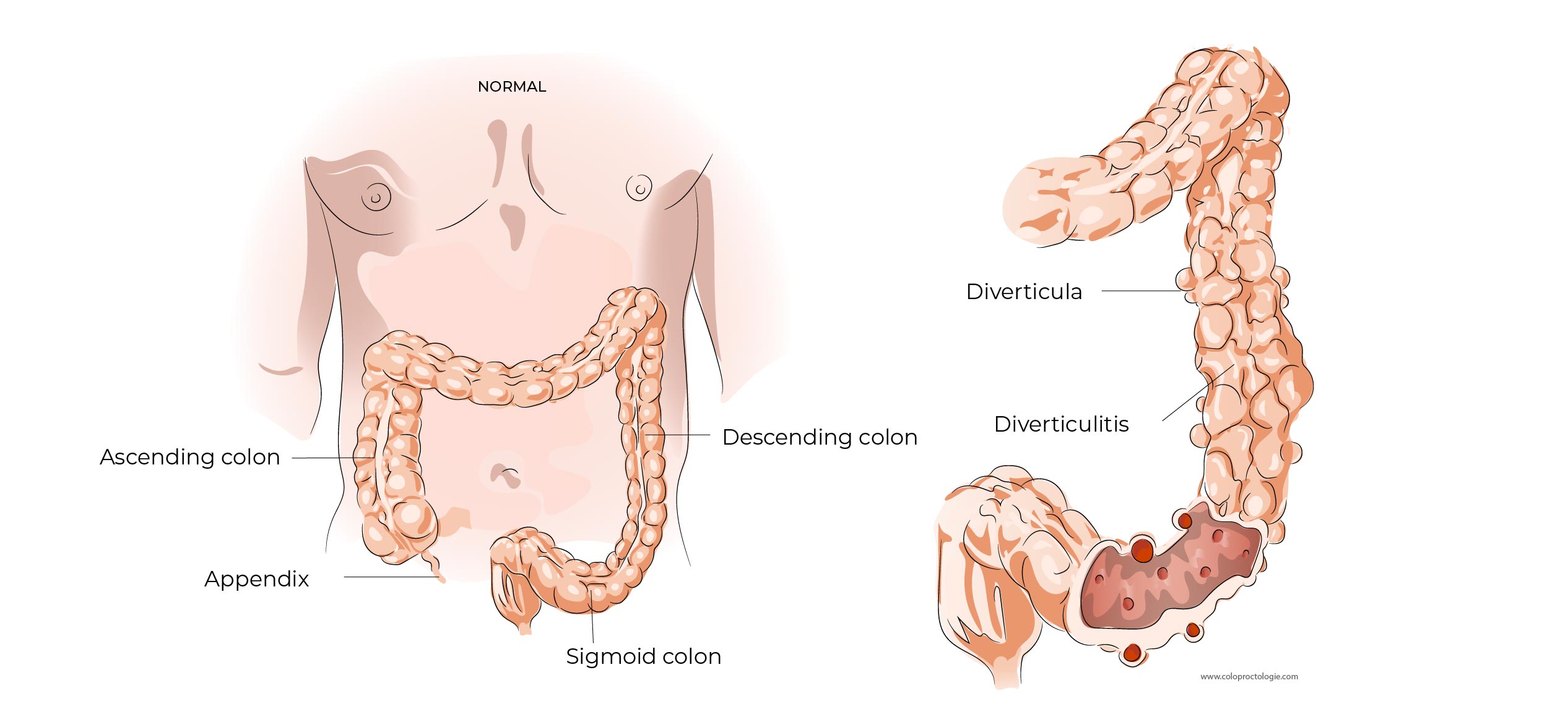
A diverticulum is a protrusion (herniation) of the mucosa and submucosa through the muscular layer, pushing out the serosa.
Diverticula can occur throughout the digestive system, from the oesophagus to the rectum. The most commonly affected segment is the sigmoid. The pressure in the colon is the highest in the sigmoid and causes the protrusion of the inner layers of the intestine through the muscular layer of the colon and causes diverticulosis.
Diverticulosis:
One speaks of diverticulosis of the colon when multiple diverticula are present.
In patients living in Europe, diverticula are, greater in numbers, smaller in size and most frequently on the left side. In Asians, living in Asia, diverticula are usually on the right side, larger in size and smaller in numbers.
Age:
– 40 years: 10% population
– 80 years: 70% population
(Eng J Med 2007; 357:2057-2066)
Diverticulitis:
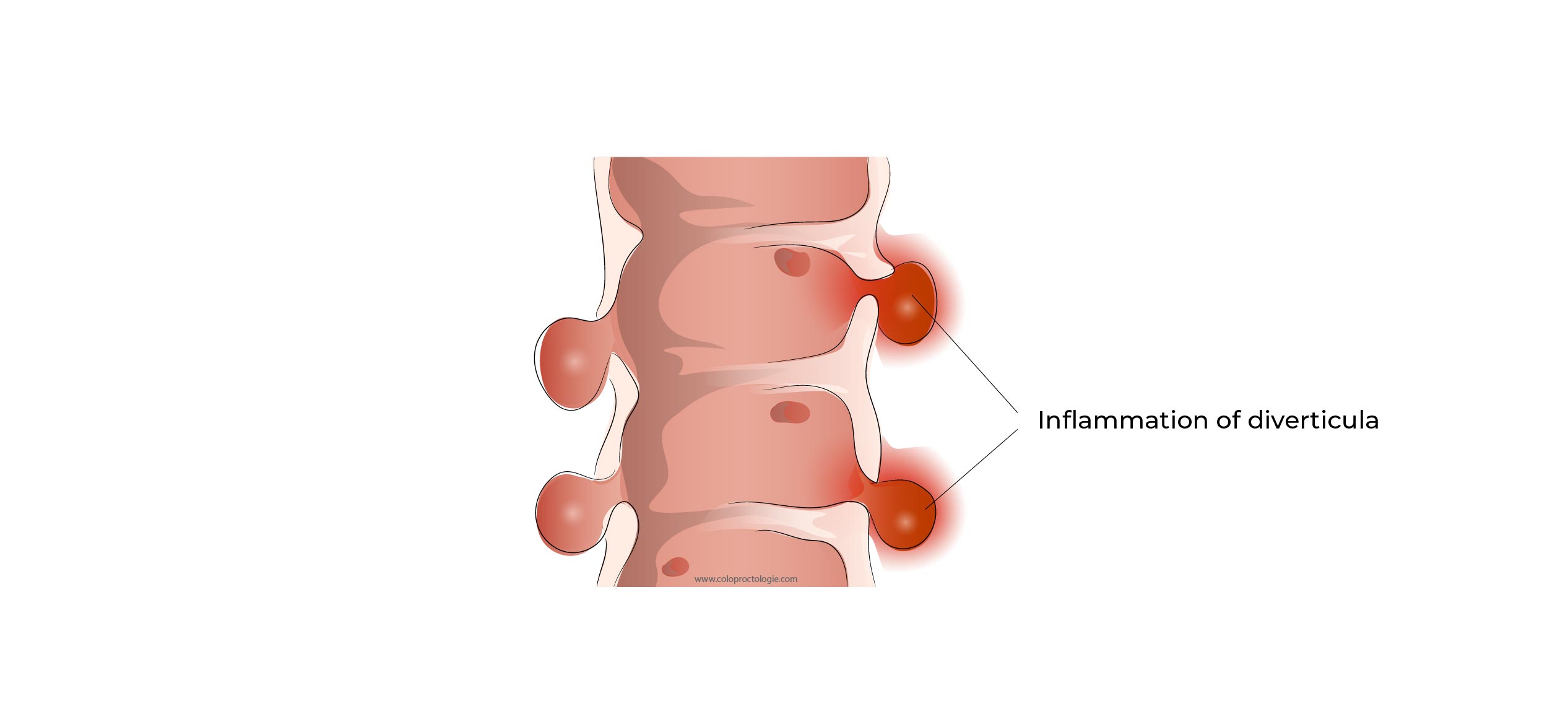
Diverticulitis of the colon is the inflammation of the mucosal and submucosal sac protruding through the muscular wall of the colon.
+/- About 5% of patients with diverticulosis develop diverticulitis.
(American Gastroenterology Association 2015).
The number of hospital admissions for diverticulitis is increasing, especially in patients between 28 and 44 years old.
(Ann sur 2009;249:210-217)
Why do I develop acute diverticulitis?
The cause of diverticulitis is not well understood. There are several hypotheses. The diverticulum is occluded by faecal debris, the trapped bacteria present in the diverticulum multiply, increasing the pressure in the diverticulum, which can lead to the development of inflammation of the wall. Low-fibre diet may also be a contributing factor to diverticulum inflammation, by singling out certain bacteria that can harm the intestinal wall.
Inflammation of diverticula can occur throughout the intestine. The colon and, in particular, the sigmoid are the most commonly affected.
What are the symptoms of diverticulosis?
- 80 – 85% of patients have no symptoms.
- Some patients will experience vague discomfort or discomfort in the lower abdomen and/or left flank.
- +/- 5-10% will develop diverticulitis.
- +/- 14/10000 a bleeding due to diverticulosis
Scand J Gastroenterol. 2019 Feb;54(2):205-209 Incidence of diverticular bleeding: a population-based study.Olafsson GD
What are the symptoms of diverticulitis of the sigmoid?
- Low-noise symptoms. Discomfort in the left half of the lower abdomen (left fossa iliaca)
- Localised abdominal pain in the (left) lower abdomen or diffuse pain throughout the lower abdomen.
- Fever, chills
- Nausea and vomiting
- Bloating in the lower abdomen
- Diarrhea – constipation
- Air/gas present during urination (pneumaturia), is a sign of a connection between the diseased colon and bladder.
What are the complications of acute sigmoid diverticulitis?
5 – 10% of patients with diverticulosis develop diverticulitis.
15% of patients with diverticulitis develop a complicated form of diverticulitis (abscess, peritonitis, obstruction…) .
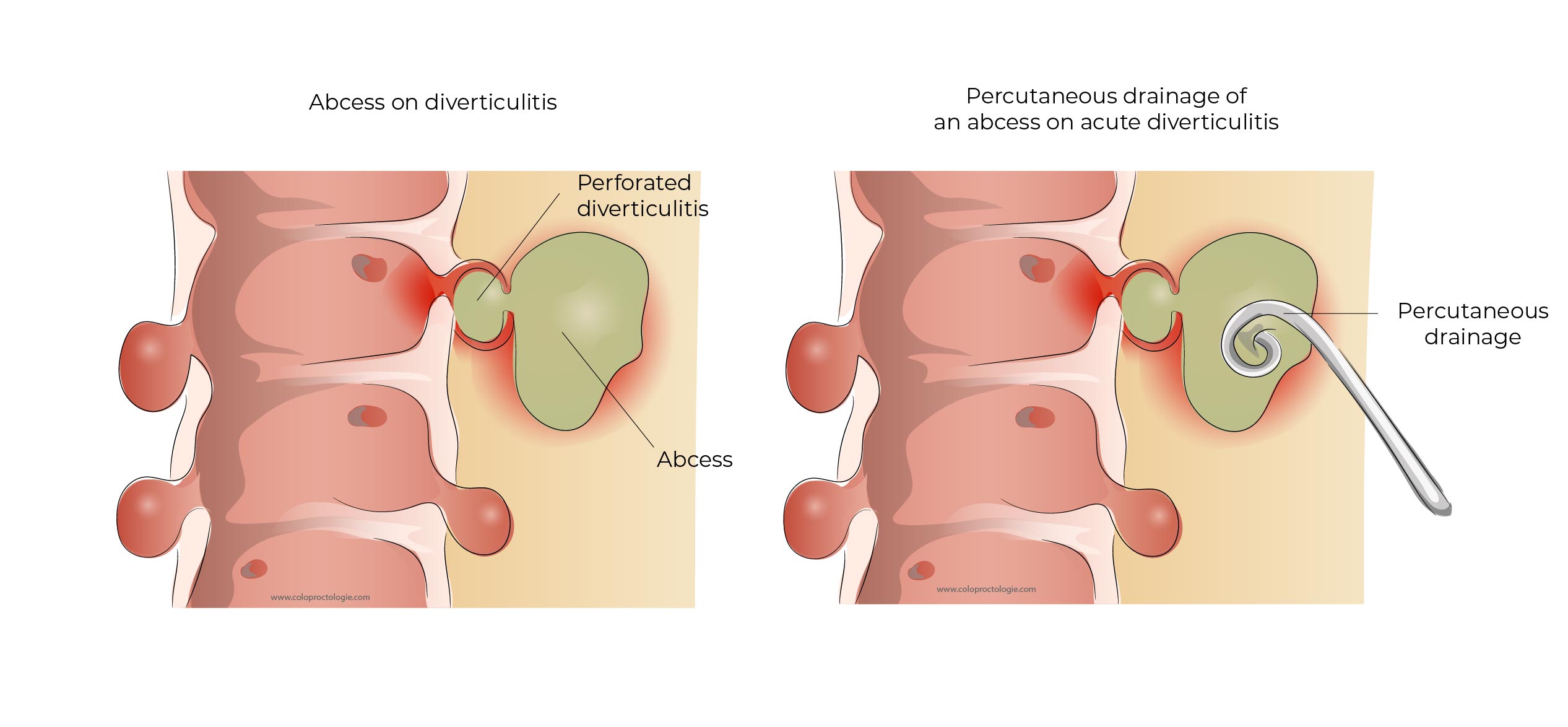
Diverticular abscess
As a result of inflammation, the diverticulum may perforate, allowing faecal material and bacteria to seep into the abdominal cavity around the diverticulum. An abscess will occur if the seeped faecal material and bacteria around the perforation, are contained by abdominal fatty tissue, abdominal wall and abdominal organs, (bowel, bladder, uterus or ovary) so that the bacteria do not infect the whole abdominal cavity.
Treatment
- A small abscess (< 3 cm) can be treated with antibiotics.
- A large abscess (> 3 cm) cannot always be treated with antibiotics and sometimes requires drainage of the abscess by percutaneous drainage by the department of radiology or surgical drainage if the abscess is inaccessible percutaneously.
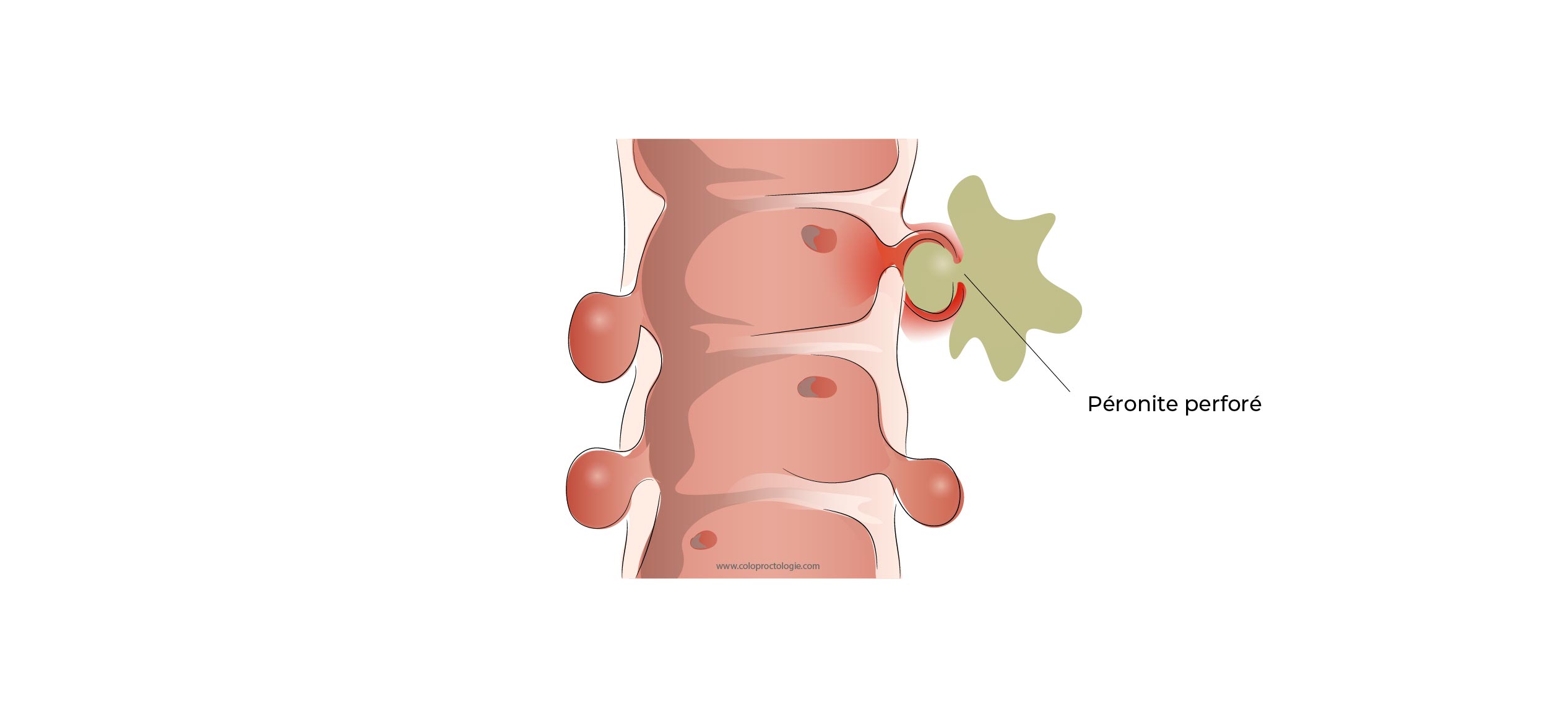
Peritonitis in acute diverticulitis
If after perforation of an inflamed diverticulum, faecal material and bacteria around the perforation are not contained and flattened by surrounding organs and tissues, they can infect the entire abdominal cavity.
Peritonitis occurs when the peritoneum of the abdominal cavity becomes infected.
Treatment
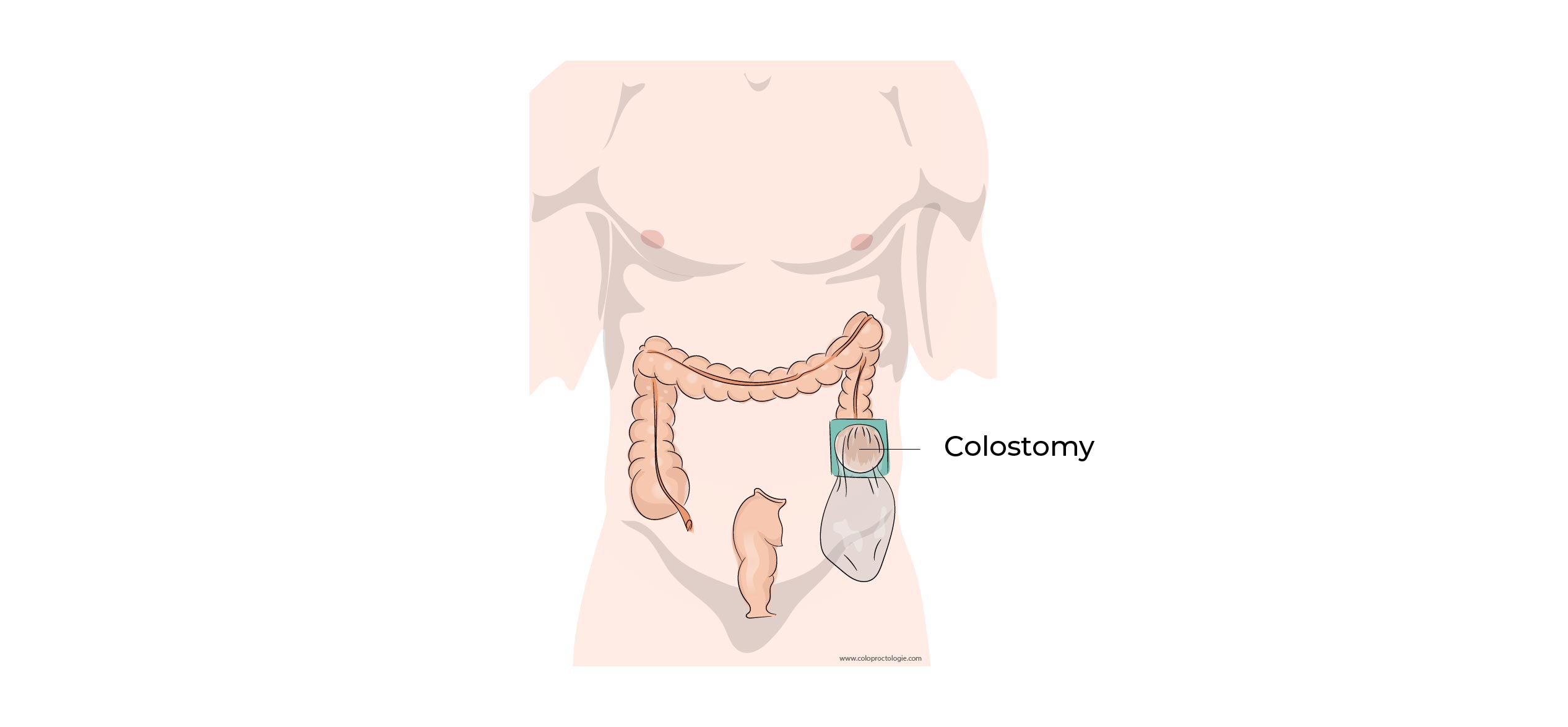
- Peritonitis is a life-threatening situation. It requires emergency surgery.
- In most cases, the resection of the diseased segment of colon is necessary and the placement of a colostomy (stoma) is often unavoidable.
(Sub) – Obstruction in chronic diverticulitis
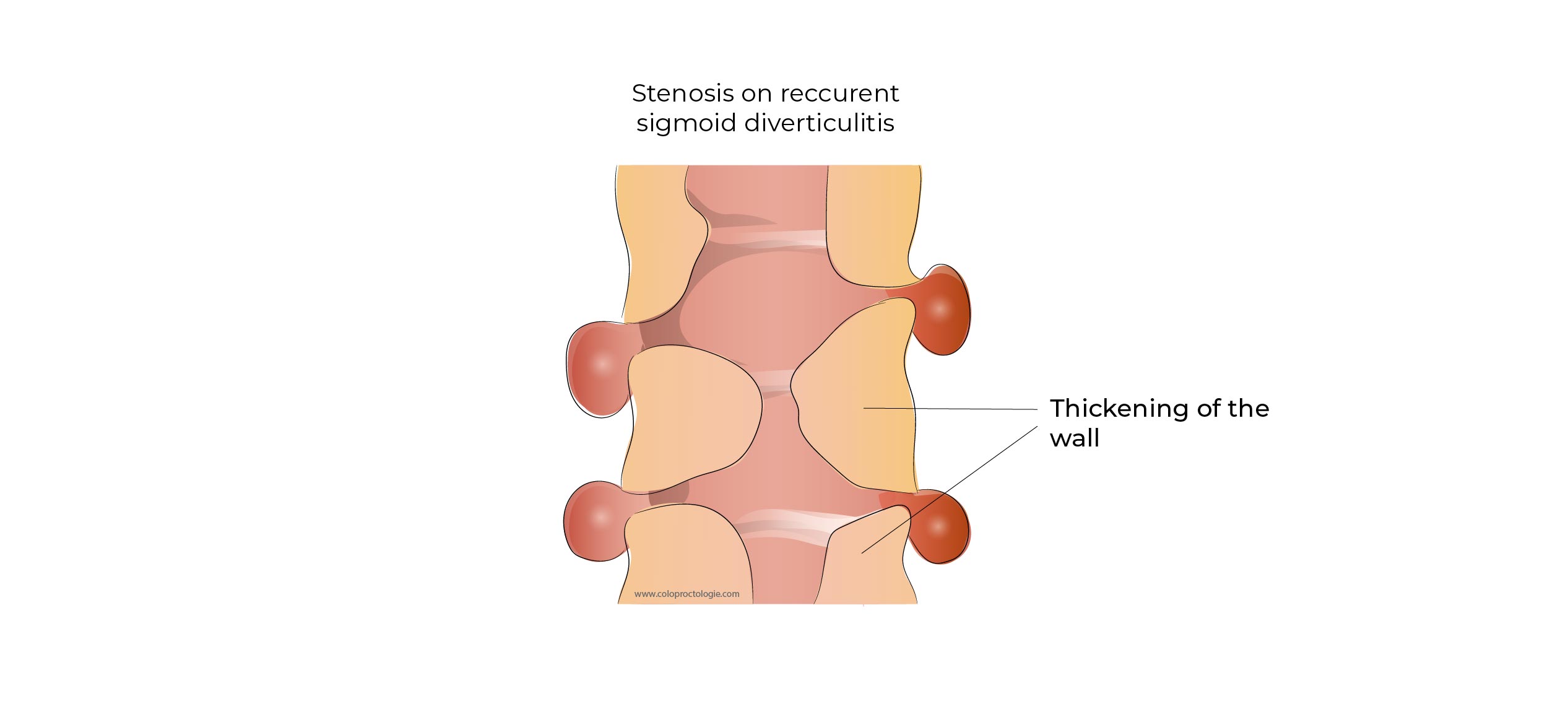
If recurrent inflammation of diverticula in a segment of the colon occurs, the segment may thicken and stiffen due to the deposition of scar tissue in the diseased segment. The bowel may lose its elasticity and mobility, and the decreased lumen of the diseased segment may clog up.
The loss of diameter of the colon and loss of mobility of the intestinal segment may block or complicate the passage of stools. As a result, patients may experience symptoms of abdominal pain, cramps, constipation or bloating.
Treatment
- If symptoms of recurrent pain or bloating are present, resection of the sigmoid is suggested.
- These patients are at risk of an acute colon obstruction or perforation if elective surgery is not performed.
Sigmoid bladder fistula
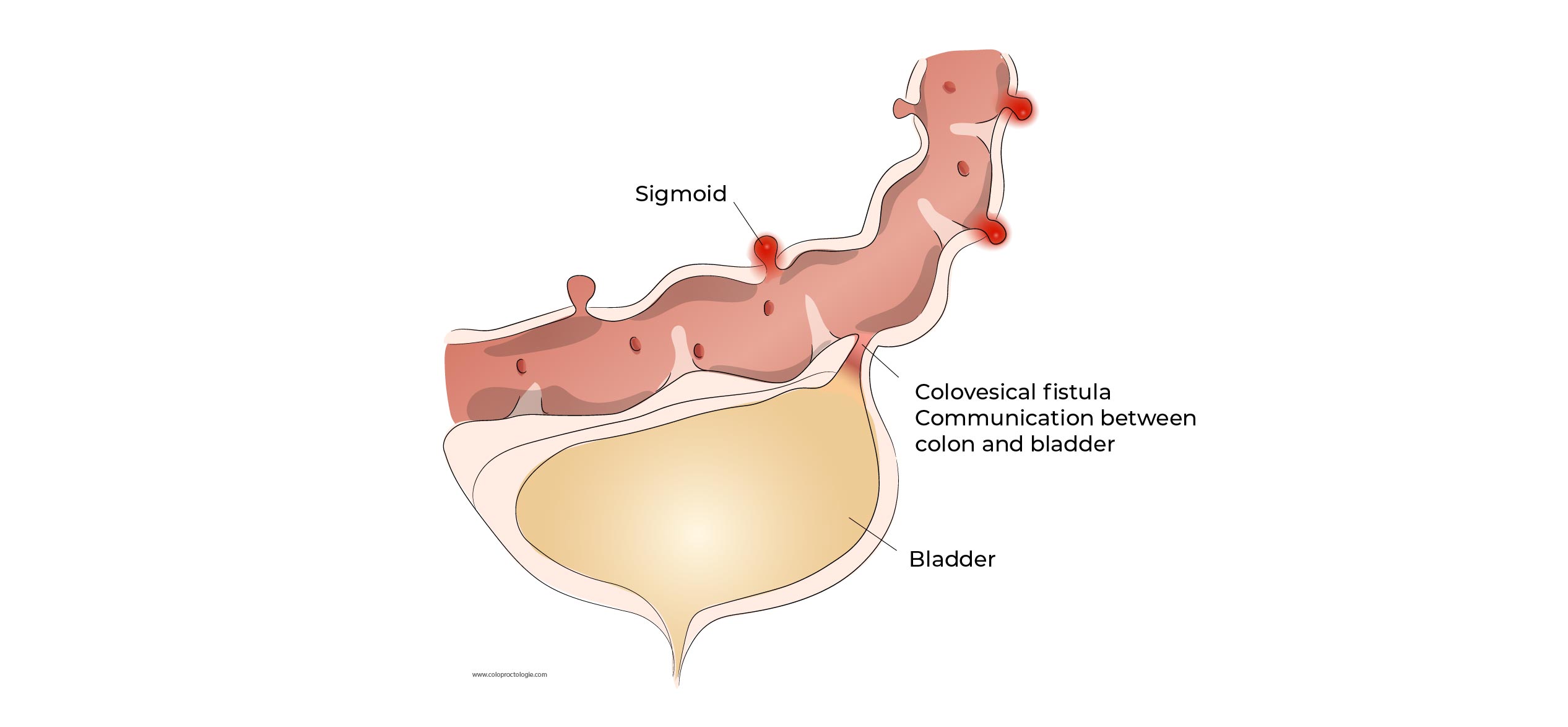
As a result of inflammation of a diverticula or an abscess in a segment of the colon ,the diverticulum or abscess may adhere to the bladder and, as a result of repeated inflammation, a pathway may form between the colon and the bladder.
As a result of bacteria migrating from the colon to the bladder, the patient will complain of recurrent urinary tract infections. The patient reports the presence of air/gas in the urine when urinating (pneumaturia).
Treatment
If a sigmoid-bladder fistula is present, a resection of the sigmoid is suggested to prevent recurrent urinary tract infections
What are the risk factors for a second episode of acute sigmoid diverticulitis?
The risk of a second episode of acute diverticulitis: 11 – 35%
Risk factors:
- The severity of the first episode
- A complicated first episode of diverticulitis with abscess.
- The younger the patient at the first episode, the higher the risk of recurrence.
Is a colonoscopy necessary after an episode of acute diverticulitis?
Après traitement d’un épisode de diverticulite aiguë , il est impératif de faire une coloscopie à froid 4 à 6 semaines après le traitement de la diverticulite afin d’exclure la présence d’une tumeur (si le patient n’a pas récemment subi une coloscopie).
4 – 6 weeks after treatment of an episode of acute diverticulitis, it is necessary to undergo a colonoscopy to rule out the presence of a tumor (if the patient has not had a colonoscopy recently).
- 2-4% of colonoscopies will demonstrate a tumor.
- 19% of colonoscopies will demonstrate polyps
- After an episode of complicated diverticulitis, 8-10% of colonoscopies will diagnose a cancer
(Ann surg 2017;265:954-959)
(Ann Surg 2014;259:263-272)
Treatment
Does diverticulosis require surgery?
The presence of diverticulosis in the colon is not an indication that surgery is the only solution.
What is the treatment of acute uncomplicated diverticulitis?
A mild episode of acute uncomplicated diverticulitis can be treated with analgesics without antibiotics and diet. In most cases, antibiotics and a light diet will be prescribed.
How to prevent recurrence of acute diverticulitis?
Neither medication nor a special diet can prevent an episode of diverticulitis. A high-fibre diet can reduce the risk of recurrence.
When is hospitalisation necessary?
A severe diverticulitis with fever, tachycardia, diffuse abdominal pain
If intolerance to liquid or oral food.
- Failure of outpatient treatment (persistent fever or increased pain),
- Persistent high white blood cell count in blood sampling (after 2-3 days)
- Immune-compromised patient or patient with severe comorbidity
- Severe pain requiring intravenous analgesics
When is surgery performed after acute diverticulitis?
The indications for surgery have changed. Two episodes of diverticulitis or one episode of diverticulitis before the age of 40 are no longer indications for surgical intervention.
Current surgical indications
- Recurrent episodes of diverticulitis over a short period of time with significant morbidity for the patient.
- Chronic (persistent) diverticulitis, despite long-term treatment with antibiotics.
- Stenosis/obstruction of the colon after repetitive episodes of diverticulitis.
- Colo-vesical fistula.
- Abscess on diverticulitis that cannot be drained percutaneously, may require surgical drainage.
- Perforation of inflamed diverticulum with diffuse severe infection (peritonitis) of the entire abdominal cavity.
What is the risk of colostomy (pouch) after a recurrent episode of acute diverticulitis?
The first episode of acute diverticulitis is usually the most severe.
The risk of a colostomy during a new episode of diverticulitis after successful treatment of a first episode of acute diverticulitis: +/- 1/2000
What surgery is performed for sigmoid diverticulitis?
Surgery involves removing the sigmoid/left colon affected by episodes of diverticulitis and reattaching the colon to the rectum.