Right colectomy
Operation
 Print this article
Print this article Download the article
Download the article Making an appointment
Making an appointmentIndications
– Right colon cancer
– Perforation of the right colon
– Right colon polyp(s)
– Right colon ischemia
– Benign tumor of the right colon
– Volvulus of the right colon
Surgery
Technique
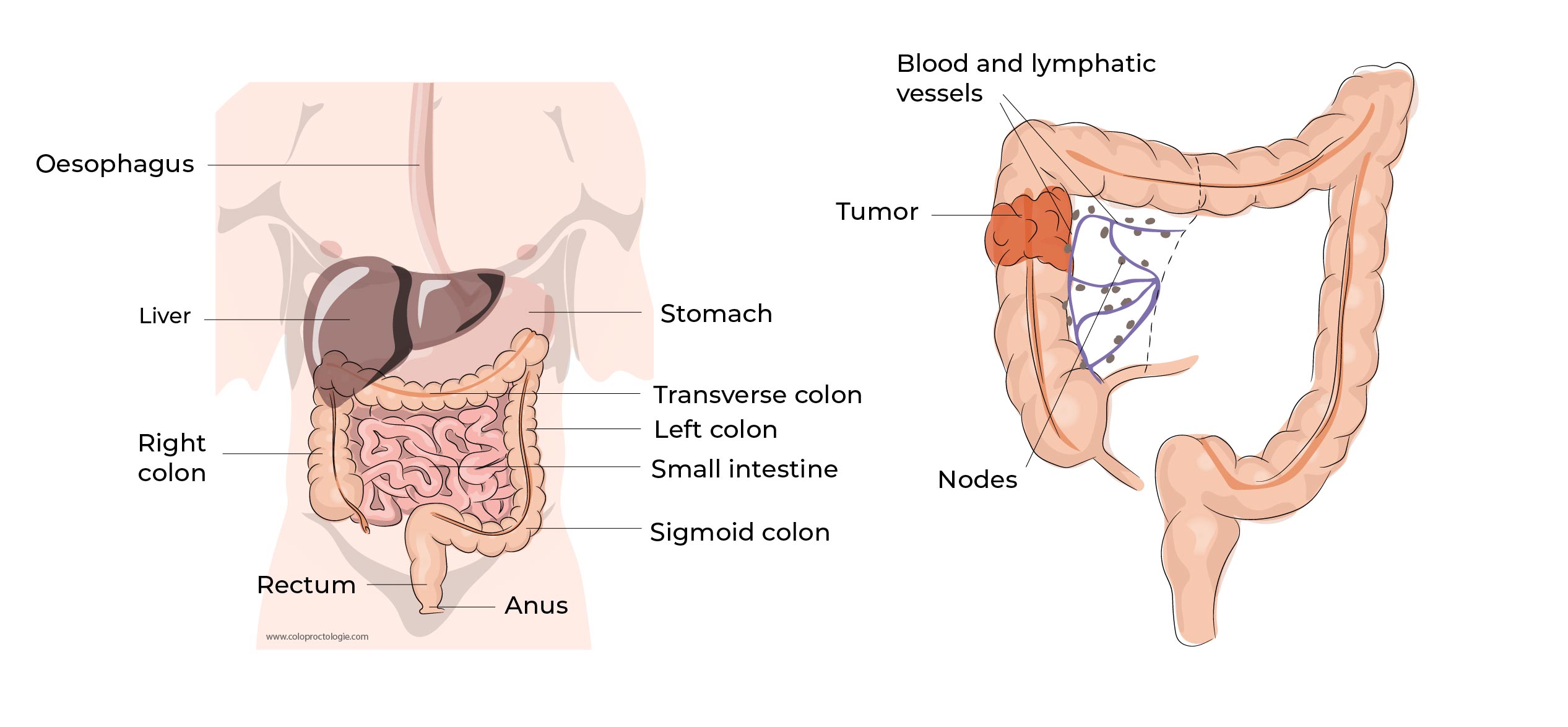
A right colectomy is the removal of the right colon (first part of the colon) up to the transverse colon (second part of the colon) and restoring the continuity by connecting the ileum (last part of the small intestine) to the transverse colon. The procedure is performed under general anesthesia.
In the first stage of the procedure, the colon is freed from its attachments all the way to the middle of the transverse part of the colon.
During this phase, the surgeon must pay attention not to injure the duodenum (first part of the bowel) and the right ureter (tube that carries urine from the kidney to the bladder).
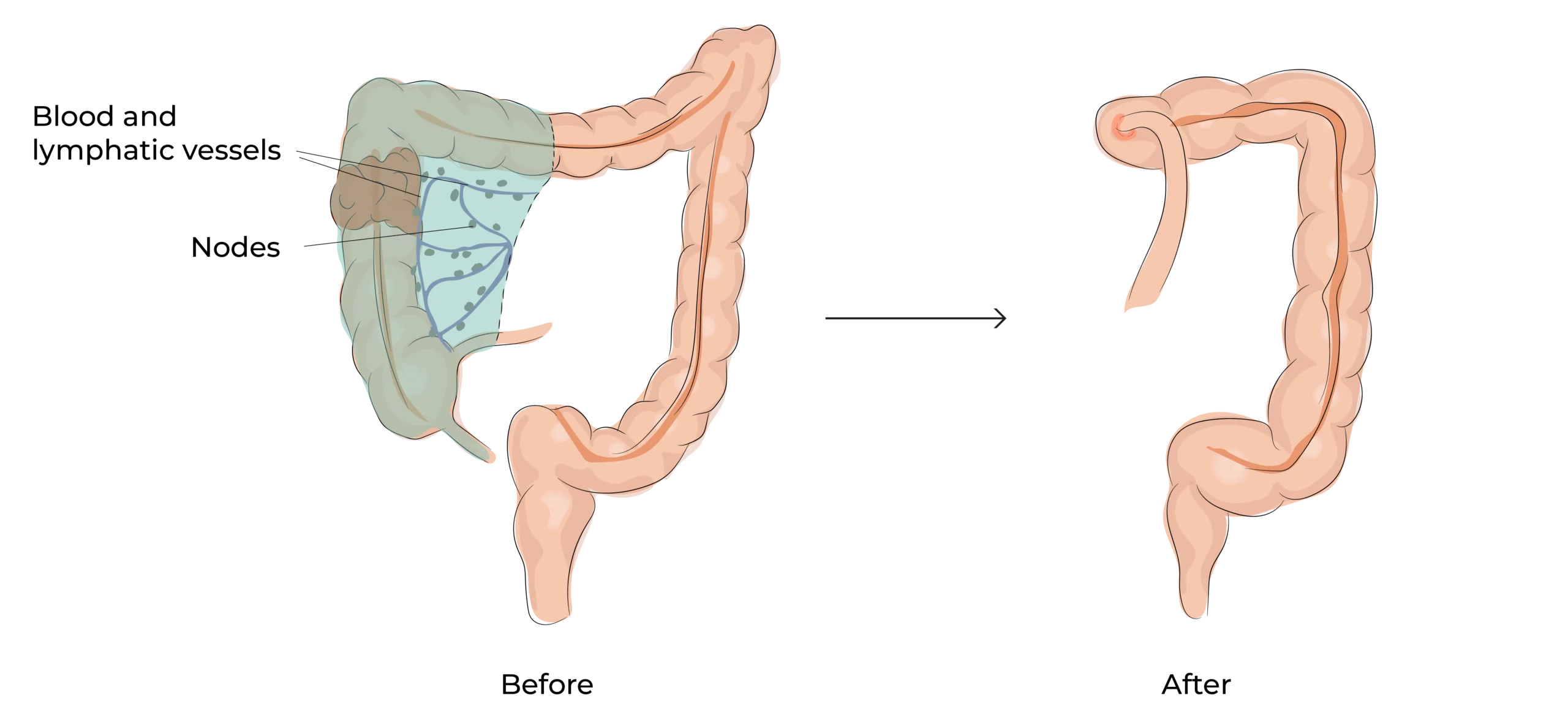
In the second stage of the procedure, the colon together with the surrounding fatty tissue containing the blood vessels and lymphatic tissue (lymph nodes) of the colon are removed , ” en block ” (in one piece).
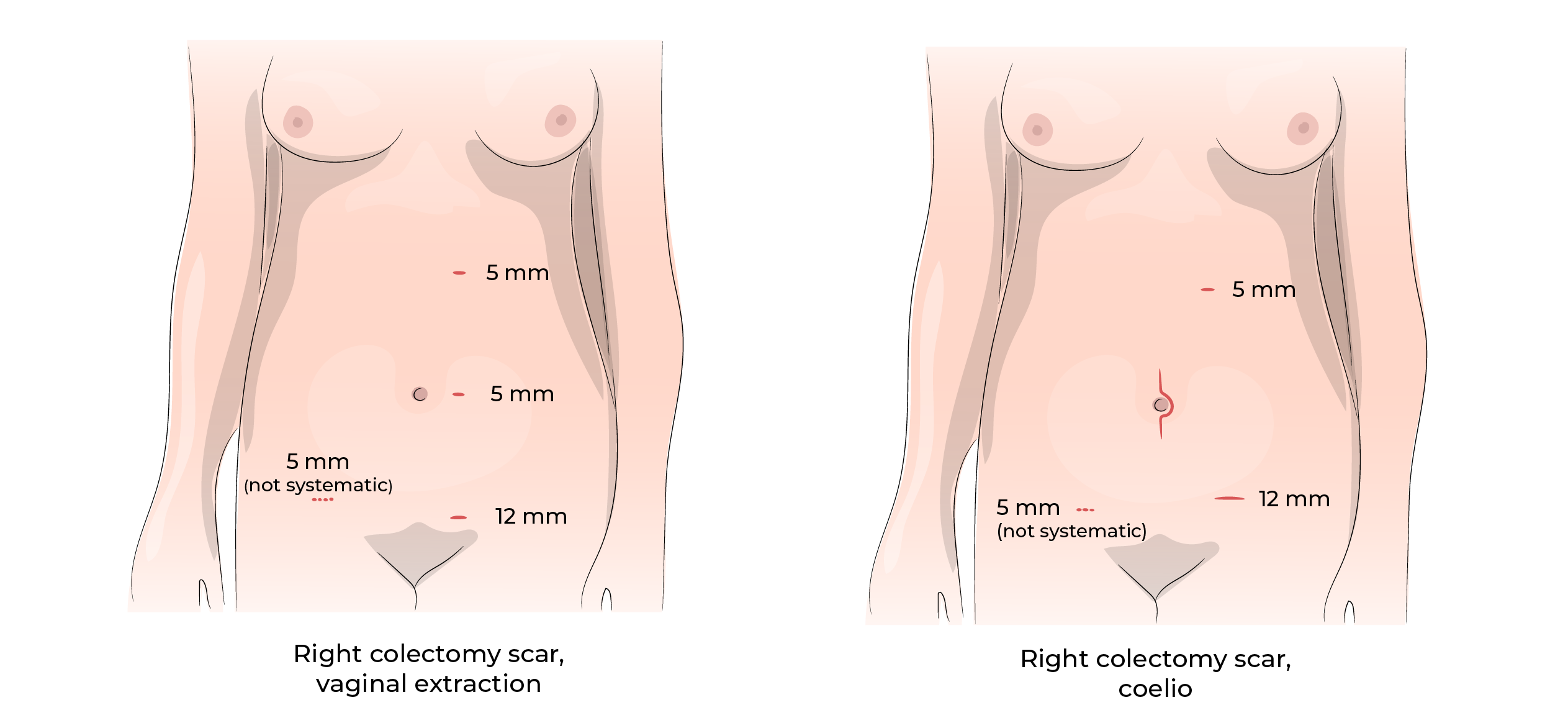
The tumor with its fatty envelope is removed from the abdominal cavity through an incision in the lower abdomen( pubic area), at the level of the umbilicus or in selected cases after consultation with the patient through the vagina.
If the extraction is performed through the vagina, the patient should abstain from sexual relations for 4 weeks. Extraction of the colon through the vagina does not alter sexual pleasure.
The removed lymphoid tissue is examined for the presence of tumor cells in the lymph nodes. The presence of tumor cells in lymph nodes is an important factor when deciding whether or not to administer adjuvant chemotherapy.(chemotherapy after surgery).
In the third stage continuity is restored by making a anastomosis (suture) between the small intestine and the transverse colon so that faeces still are evacuated through the anus.
The anastomosis/suture/suture is usually performed in the abdominal cavity with keyhole surgery.
Laparoscopy (keyhole surgery) – open surgery
Advantages:
- Less pain.
- Faster recovery.
- Aesthetic.
- Less wound infection.
- Less incisional hernias
Laparoscopy may not be possible when:
- Many adhesions in the abdominal cavity.
- Anatomy difficult to recognize due to multiple previous procedures.
- Anatomy difficult to recognize due to severe inflammation.
- In case of bleeding that is difficult to control with laparoscopy.
- In case of infiltration of the tumor into adjacent organs.
- Important intra-abdominal obesity (male).
Complications
Factors that increase the risk of complications:
- Male gender
- With increasing age
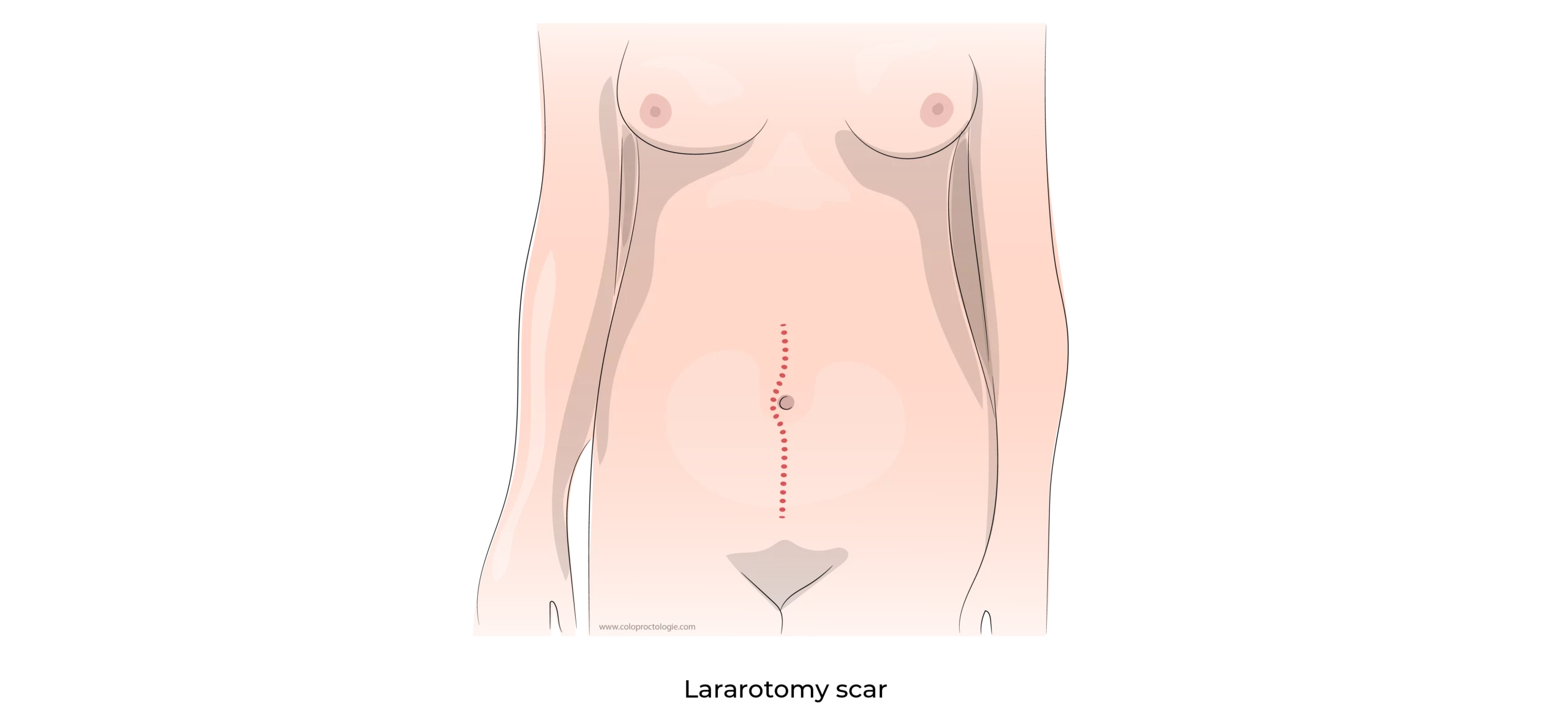
- Open surgery/laparotomy
- Obesity
- Malnutrition
- Associated diseases of the patient: diabetes, cardiovascular diseases, pulmonary diseases, etc.
Leakage at the suture/suture and fistula
Incidence : 1,8 – 8 %
- If the suture does not heal, an opening may develop on the suture between the colon and small intestine. As a result of the opening between the two ends, stool may leak into the abdominal cavity and form an abscess locally or cause a general infection of the abdominal cavity (peritonitis).
- The risk exists mainly during the first 2 weeks after surgery.
- A fistula is a surgical emergency that may require percutaneous drainage of the abscess or resection of the newly constructed anastomosis and placement of a stoma.
A stoma is a surgical procedure in which the bowel is sutured through the abdominal wall earth the skin so that the fecal matter is discharged via in a pouch / bag attached to the skin.
Occlusion – obstruction of the bowel
Incidence : < 9 % after laparotomy for abdominal surgery
Adhesions of the small intestine are the main causes of postoperative obstruction. If the obstruction does not clear up spontaneously, surgery may be necessary. Laparoscopic surgery requires less traumatic manipulation of the bowel and causes fewer adhesions. The risk of obstructions is much lower after laparoscopy (keyhole surgery) than after laparotomy (open abdominal surgery).
Mortality
Incidence : 1,1 – 2,3 %
Wound infection
Incidence : 10 %
Wound infection is common after colon surgery because the colon contains millions/billions of bacteria that may infect the wound. The risk is higher in open surgery than in laparoscopic surgery.
Among other factors, obesity, malnutrition, diabetes and corticosteroids increase the risk of an infection.
Incisional hernia
Laparoscopy : incidence : 7 %*
Open laparotomy : incidence : 22,4%*
Wound infection, obesity, malnutrition, diabetes and chronic use of corticosteroids are factors that increase the risk of incisional hernia.
Postoperative bleeding
Patients at risk are those requiring anticoagulation medication for cardiovascular disease or those with bleeding disorders.
- Bleeding at the anastomosis (suture) : 6,4%*
In most cases, the bleeding stops spontaneously. Treatment by endoscopy (colonoscopy) is rarely necessary.
- Intra-abdominal hemorrhage: rare complication.
Ileus – bowel paralysis
Incidence : 6,8 %*
After abdominal surgery, the bowel may temporarily lose its ability to contract and expel food, this is called an ileus.
The bowel dilates and the patient can no longer feed. An ileus manifested by discomfort due to the dilated abdomen that may or may not be accompanied by vomiting.
The bowel dilates and the patient can no longer feed. An ileus manifested by discomfort due to the dilated abdomen that may or may not be accompanied by vomiting.
Treatment consists of resting the bowel, inserting a nasogastric probe through which the stomach and bowel are decompressed and stopping morphine analgesics,. The bowel spontaneously returns to normal after 1 to 10 days. On average, postoperative ileus prolongs hospitalization by 4 days. Ileus is more common after laparotomy than after laparoscopy.
Int J Colorectal dis 2016 Sep31 (9) 1619-24. Colorectal dis 2018 Jun19 Ann Gastroenterol Surg 2018 May :2(3);220-230
JSLS 2016 Oct -Dec (20)4
J gastroenterol 2014;49:1047-55)
(3 – 30%) Robert L Smith : Wound infection after elective surgery. Ann Surg 2004. May 239 (5) 599-607
(3 years) J.R.A Skipworth Incisional hernia rates following laparoscopic colorectal resection Int. J. Of Surgery Vol8,6, 2010, 470-473
(3 years) Fink C Br J Surg 2014 Jan ;101(2):51-4.
Normal – abnormal symptoms
Normal symptoms
In normal conditions, pain is well controlled with paracetamol (Dafalgan®), NSAIDs (anti-inflammatories) or morphine (Tradonal®…) and pain symptoms diminish over time.
- Abdominal bloating gradually decreases postoperatively for 2 weeks.
- Irregular bowel movements. With a low-residue diet, we produce fewer stools. 1 stool every 3 days may be normal. When a normal diet is introduced, it is normal to have loose and small amounts of stools at a higher frequency for the first few weeks – months.
- Shoulder pain (24-48 hours) due to irritation from the CO 2-gas injected during the laparoscopic procedure.
- Urinary retention may occur in the first hours after the procedure. Temporary placement of a urinary catheter may be necessary.
- Nausea and vomiting (24-48 hours) may occur. Adolescents and especially young women are more affected.
- Hardening and pain at the level of the scar. The wound may feel hard for several weeks/months.
- Pain is often aggravated by sudden movements of the abdominal wall laughing, coughing, sneezing,….).
- Pain will usually be most pronounced at the level of the extraction scar ( scar along which the piece of colon was removed.
- On returning home, the joy of returning home, is often followed by an increase in fatigue and sometimes a drop in morale.
Abnormal symptoms
If certain symptoms seem abnormal to you contact your doctor.
- Postoperative abdominal pain that does not subside but increases with time.
- Persistent fever.
- Inability to eat due to nausea and vomiting.
- Increased bloating.
If this is not possible, you can contact your surgeon.
If you are unable to contact your GP or your surgeon, go to the emergency department at St Elizabeth Hospital in Uccle.
Functional outcomes: Bowel movements and sexual function
Bowel movement
Upon resection (removal) of the right colon, the length of the colon is reduced.
This reduces the postoperative ability to reabsorb water from the stools, so bowel movements may be softer and even liquid immediately after surgery (diarrhea).
The remaining colon has enough length to adapt and absorb more water, in subsequent weeks and months the stools can return to a normal consistency.
Sexual function
Right colectomy has no direct impact on sexual function either in men or women.