Operation
 Print this article
Print this article Download the article
Download the article Making an appointment
Making an appointmentIndications
– Biliary colic
– Acute cholecystitis
– After jaundice due to gallstones
– Pancreatitis due to gallstones
– Gallbladder polyp
Surgery
Technique:
The abdominal cavity is first insufflated with a gas (CO2) to increase space in the abdominal cavity and make keyhole surgery (laparoscopy). Four small holes are created through which ports (trocarts) are inserted. A trocart (port) is a cylinder made of metal or hard plastic placed through the abdominal wall. Instruments necessary to perform the operation are inserted through the trocarts (ports). Three 5mm and one 10mm trocart are inserted.
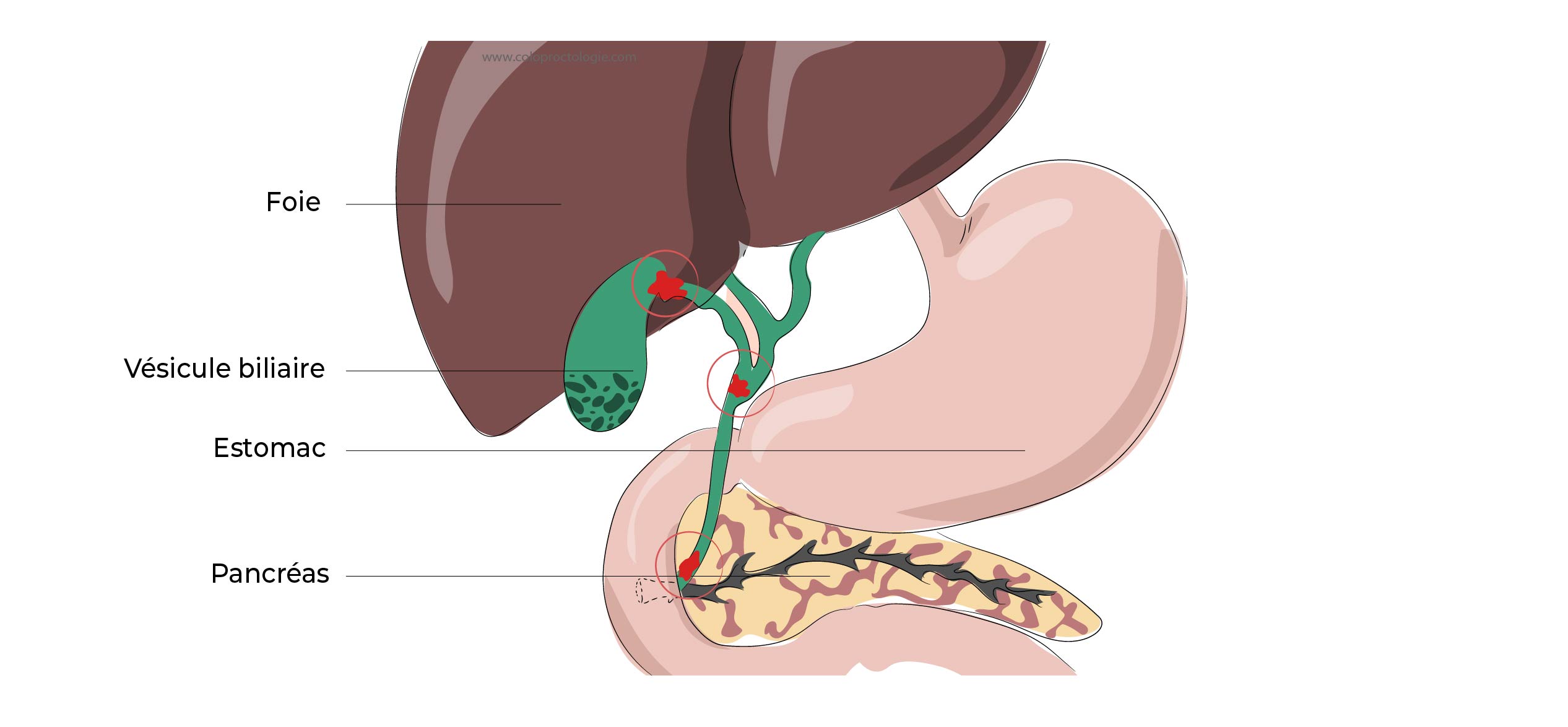
During surgery, the gallbladder is detached from the liver using electrocoagulation, an electric current that burns the adherent tissue between the liver and gallbladder.
The two main structures that the surgeon needs to identify during the procedure is the duct, which connects the gallbladder to the main bile duct (cystic duct) and the artery that feeds the gallbladder. The cystic duct (tube connecting gallbladder to the main bile duct) is closed with one or more clips to prevent leakage of bile through the bile stump. It is important that the main bile duct is not damaged during the procedure. Once the gallbladder has been detached from these structures, it will be removed through the wound at the umbilicus.

Laparoscopy (keyhole surgery) – open surgery
Advantages:
- Less pain
- Faster recovery
- Aesthetic
- Less wound infection
- Less incisional hernias

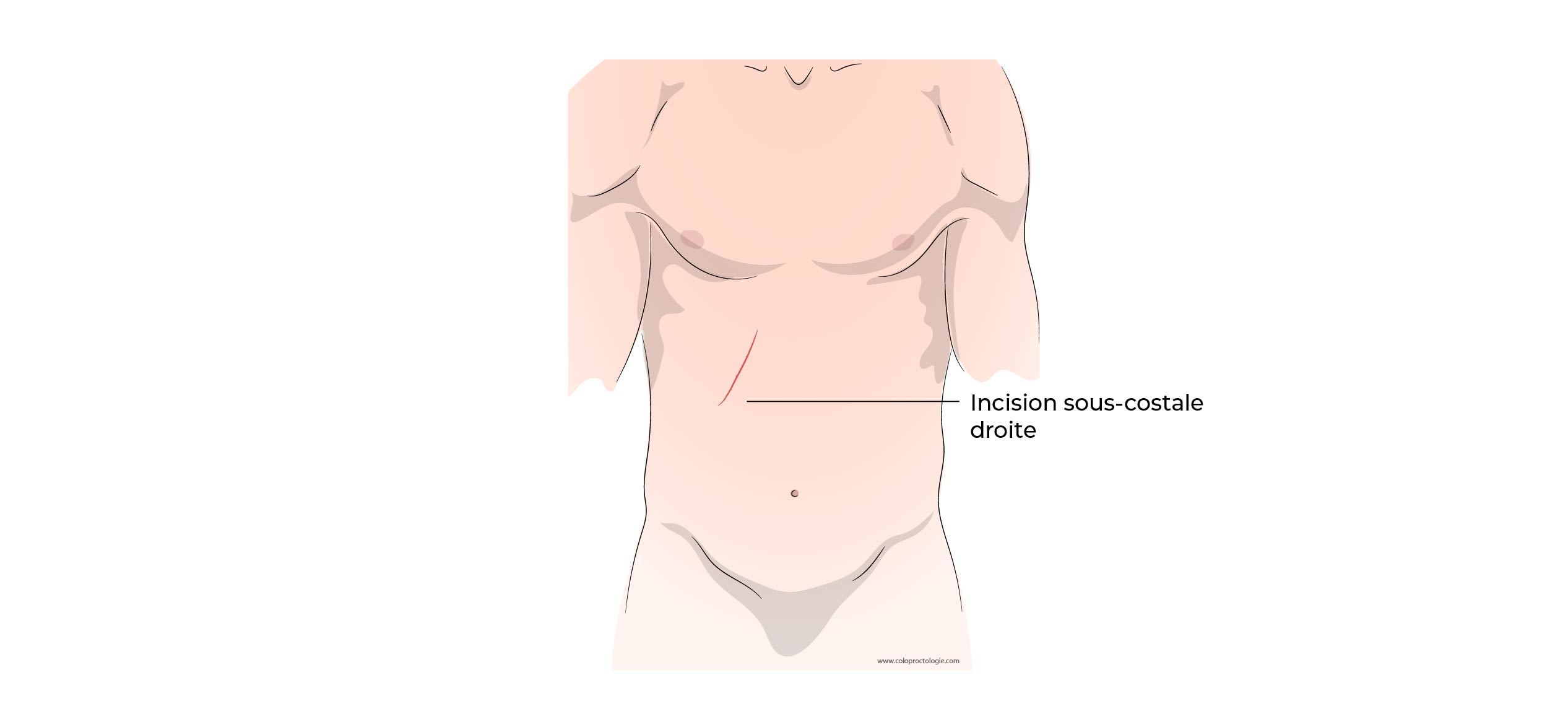
Laparotomy – open abdominal surgery
Laparoscopy is sometimes not possible in case of :
- Many adhesions in the abdominal cavity .
- Anatomy difficult to recognize due to multiple previous procedures.
- Anatomy difficult to recognize due to severe inflammation of the gallbladder and the surrounding tissues.
- In case of bleeding that is difficult to control with laparoscopy.
Complications
Hemorrhage – bleeding:
- Incidence : 0,11 – 1,97%
Wound infection (keyhole surgery):
- Incidence : Rare
Incisional hernia:
- Incidence : +/- 1,5%
Abscess:
- Incidence : 0,14 – 0,35 %
Bile leak:
- Incidence : 0,3 – 0,9 %
Bile duct injury:
- Incidence : 0,26 – 0,6 %
Bowel injury:
- Incidence : 0,14 – 0,35 %
Sofie Anne-Marie Skovbo Jensen Low long term incisional incidence of incisional hernia after cholecystectomy: A systematic review with meta-analysis Surgery 2021 Feb17
Peter. D Thurley Laparoscopic imaging cholecystectomy: Postoperative imaging:AJR:191, September 2008
Wound infection
- Wound infection can be recognised by increasing redness, swelling and pain at the level of the wound. If an abscess develops, the infected wound may fluctuate and the patient may develop fever.
- In case of a skin infection, treatment consists of oral antibiotics.
- If an abscess develops, it will be incised and drained. Daily wound care with a wheeze may be required.
Bile duct leak or injury
- In case of a bile leakage/injury, bile partially escapes into the abdominal cavity. It may accumulate in the abdominal cavity, infect and form an abscess. Usually the leakage occurs at the level of the stump of the truncated bile duct.
- If the bile leakage stops spontaneously, treatment may be limited to percutaneous drainage.
- If the bile leakage is significant, a stent (tube) is placed endoscopically (ERCP) in the bile duct. The purpose of the stent (tube) is to cover the wound to prevent bile from flowing into the abdominal cavity and to speed up wound healing. After 3 months, the stent (tube) is removed endoscopically.
- If the main bile duct connecting the liver to the intestine is completely slit, surgery will be needed to allow bile to flow back into the intestine.
Normal – abnormal symptoms
Normal symptoms
In normal circumstances, pain is easily controlled with paracetamol (Dafalgan®) NSAIDs (anti-inflammatories) or morphine (Tradonal®…) and pain symptoms diminish over time :
- Nausea and vomiting (24–48 hours) may occur. Adolescents and especially young women are more affected.
- Hardening and pain at the level of the scar. The wound may feel hard for several weeks.
- Shoulder pain (24-48 hours) due to irritation from the CO 2-gas injected during the laparoscopic procedure.
- Pain is often aggravated by sudden movements of the abdominal wall laughing, coughing, sneezing,…
- Urinary retention may occur in the first hours after the procedure. Temporary placement of a urinary catheter may be necessary.
- On returning home, the joy of returning home, is often followed by an increase in fatigue and sometimes a drop in morale.
-
Decreasing pain in the right upper abdomen (right hypochondrium).
Abnormal symptoms
If certain symptoms seem abnormal to you contact your doctor
- Postoperative abdominal pain that does not decrease but increases with time
- Persistent fever
- Jaundice
- Inability to eat due to nausea and vomiting
- Increased bloating
If this is not possible, you can contact avec your surgeon.
If you are unable to contact your GP or your surgeon, go to the uremergency department at St Elizabeth Hospital in Uccle.
Functional Results
Diarrhea after gallbladder resection (cholecystectomy)
10 à 15% of patients experience diarrhea, sometimes accompanied by bloating, poor digestion or upper abdominal (epigastric) pain.
In most cases, symptoms disappear soon after surgery.
If symptoms persist, you should consult your GP (general practician) or surgeon.