Proctologische pathologie
Anale fissuur
 Artikel afdrukken
Artikel afdrukken Artikel downloaden
Artikel downloaden Maak een afspraak
Maak een afspraakPathologie
Wat is een anale fissuur?
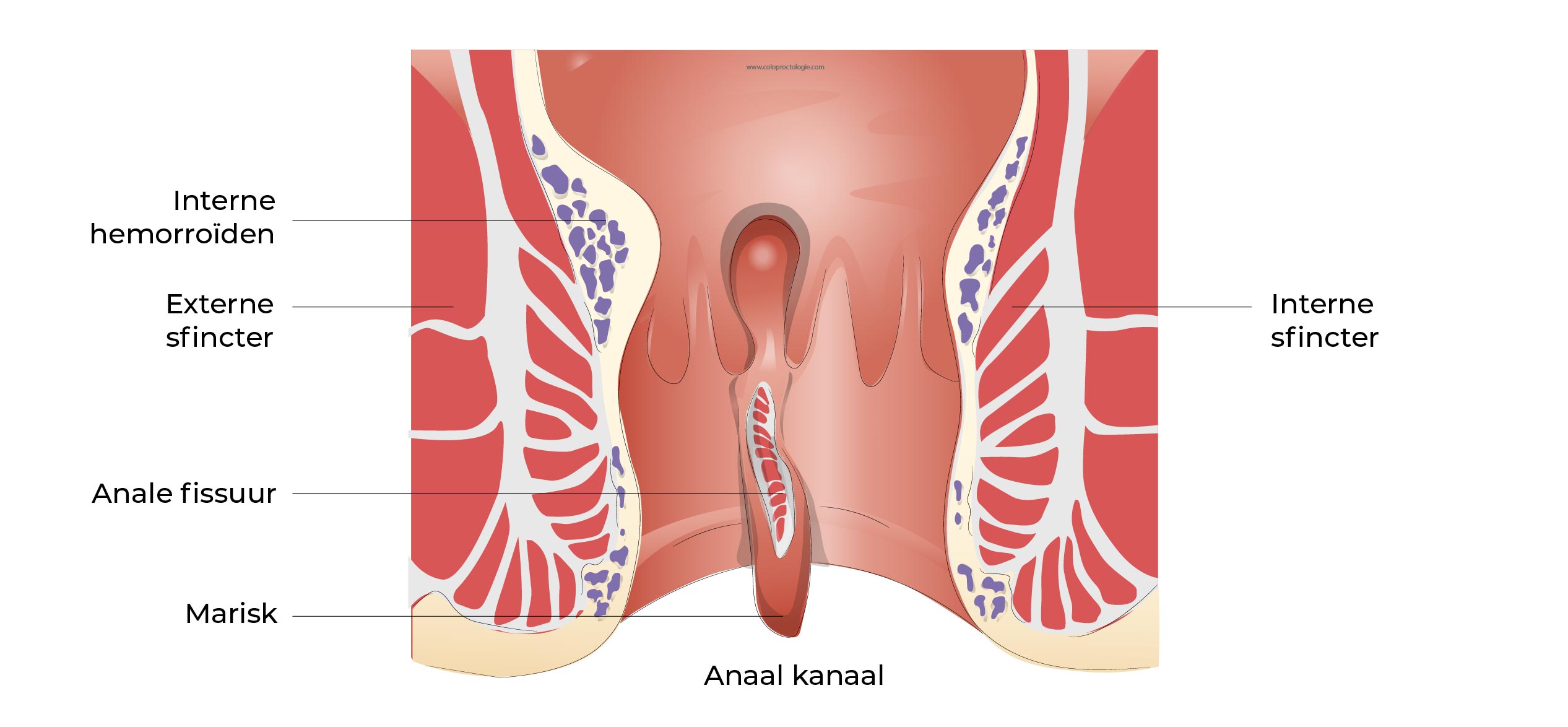
- Een anale fissuur is een oppervlakkige scheur (een wonde) in de bekleding (mucosa/ slijmvlies) van het anaal kanaal. De fissuur is vaak niet zichtbaar van buitenaf.
- Gemiddelde leeftijd 39,9 jaar.
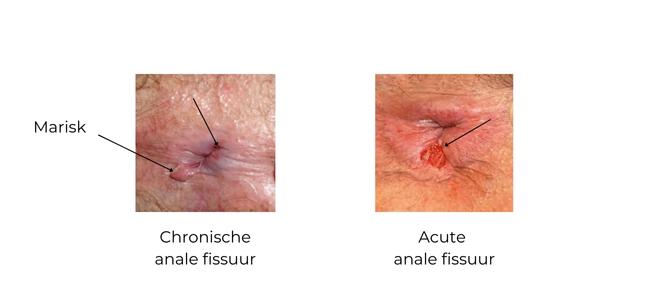
Type anale fissuur:
– Acute anale fissuur: minder dan 4 weken aanwezig.
– Chronische anale fissuur: recidiverende fissuur, langer dan 4 weken aanwezig.
Wat zijn de symptomen van een anale fissuur?
- Anale pijn (90.8%) tijdens de ontlasting die tot 2-3 uur kan aanhouden. Als gevolg van de pijn heeft de patiënt angst om naar het toilet te gaan en te ontlasten. De patiënt heeft de neiging om de ontlasting uit te stellen en verergert zo de constipatie waardoor de pijn bij de ontlasting nog toeneemt.
- Brandend gevoel na de ontlasting.
- Bloedverlies (71.4%) na ontlasting op toiletpapier.
(Hanalel et al Dis Colon Rectum 1997; 40 (2):229-233)
Alle 3 symptomen kunnen met wisselende frequentie en intensiteit voorkomen.
De symptomen zijn meer uitgesproken bij harde ontlasting en tijdens periodes van constipatie.
Soms kan zich een abces vormen achter de fissuur (retro-fissuraal abces). De patiënt klaagt dan over intermittent vuilverlies.
Waarom ontwikkel je een anale fissuur?
De oorsprong van een anale fissuur is niet altijd bekend.
In de meeste gevallen ontstaat een anale fissuur als gevolg van een trauma aan het slijmvlies (de oppervlaktelaag) van het anale kanaal.
Als gevolg van de pijn trekt de spier van de anus (sluitspier) samen (spasme). Dit verhoogt de pijn en vermindert de bloedtoevoer naar de wond, waardoor de fissuur niet kan genezen.
Als gevolg van de pijn ontstaat er een vicieuze cirkel, de patiënt stelt de ontlasting uit, de ontlasting blijft langer in de dikke darm en wordt harder omdat er meer water uit de stoelgang in de dikke darm wordt onttrokken… De hardere stoelgang (constipatie) kwetst wederom de anale fissuur waardoor deze niet kan helen en verhoogd de pijn bij ontlasting.
Trauma:
– Constipatie
– Traumatische perineale hygiëne (traumatisch wrijven met toiletpapier)
– Seksuele praktijken (anale penetratie, vreemd lichaam)
In een minderheid van de gevallen kan de oorsprong te wijten zijn aan een ontstekingsziekte van de dikke darm zoals de ziekte van Crohn, een seksueel overdraagbare aandoening of een tumor van het anale kanaal.
Hoe wordt de diagnose van een anale fissuur gesteld?
De diagnose wordt gesteld op basis van de anamnese (gesprek met de patiënt) en het proctologisch onderzoek.
De pijn in het anale kanaal is zeer uitgesproken en inspectie van het perineum is soms voldoende. Een endoscopisch onderzoek is zelden nodig of wordt niet uitgevoerd omdat het te pijnlijk is.
Wanneer de fissuur lange tijd aanwezig is, kan een zwelling van het slijmvlies aan de rand van de fissuur zichtbaar zijn, die verkeerdelijk kan aanzien worden voor een aambei.
De meeste fissuren bevinden zich op het achterste deel van de anale sluitspier en in mindere mate op het voorste deel.
Als de plaats van de fissuur afwijkt of als er sprake is van meerdere fissuren, moet er aan andere oorzaken van anale fissuren gedacht worden. (Crohn’s, seksueel overdraagbare aandoeningen, tumoren…)
Is een anale fissuur gevaarlijk?
Een anale fissuur verhoogd niet het risico op kanker.
Een ulcus (wonde) in het anaal kanaal dat blijft bestaan ondanks behandeling, moet worden onderzocht en zo nodig moet een biopsie kwaadaardigheid uitsluiten. Een fissuur met een atypische locatie kan ook verdacht zijn en vereist verder onderzoek.
Als een bloeding deel uitmaakt van de symptomen, zal afhankelijk van de leeftijd (ouder dan 50 jaar) of van de familiale voorgeschiedenis, een colonoscopie worden aangevraagd nadat de anale fissuur genezen is.
Wat kan ik doen om een anale fissuur te voorkomen?
-
Constipatie voorkomen
De ontlasting niet ophouden, hoe langer de ontlasting in het rectum en colon blijft hoe meer heropname van water uit de stoelgang en zodoende hardere ontlasting.
Ontlasting niet ophouden tijdens het reizen (vliegtuig, trein, werkplaats…)
- Vezelrijke voeding en voldoende hydratatie (1,5-2 l per dag).
- Gebruik indien nodig milde laxeermiddelen zoals Lansoyl®.
- Lichamelijke oefening om de overgang te stimuleren.
- Vermijd agressieve anale hygiëne (niet te hard wrijven): zacht toiletpapier.
Behandeling
Wat zijn de mogelijke conservatieve behandelingen?
In de meeste gevallen kan een anale fissuur zonder operatie worden behandeld.
De behandeling bestaat uit het veranderen van de consistentie van de ontlasting, het verminderen van constipatie of diarree, het verminderen van pijn en het bevorderen van de bloedcirculatie in de wond om de vicieuze cirkel te doorbreken.
Lossere ontlasting
- Vezelrijke voeding en voldoende hydratatie: 1,5-2l.
- Vezelsupplementen in de voeding.
Laxeermiddelen
- Paraffine (Lansoyl® 3x/dag: één lepel 15 min. voor de maaltijd)
- Indien nodig macrogol (Movicol®) sachets 2-3x/dag
- Lichamelijke oefeningen om de transit in de darm te stimuleren.
Behandeling van pijn
- Zitbad met warm water 10-20 minuten, vermindert de pijn en ontspant de anale sluitspier.
- Pijnstillend:
– Paracetamol 1gr 3-4x/dag. (Dafalgan®…)
– Niet-steroïde anti-inflammatoire middelen (Brufen® 400mg 3x/dag, Cataflam®, Voltaren®, Diclofenac®…)
– Morphinique indien nodig (Tradonal Odis 50mg…)
Crème/zalf
→ Xylocaïne 5% gel:
– Verdovende zalf die in het anaal kanaal moet worden aangebracht (op en rond de fissuur).
– 3-4x/dag aanbrengen
→ Diltiazem en Isosorbidedinitrate op basis van lokale zalf:
Voorbeelden: Rectogesic®, magistral bereiding…
– Het aanbrengen van de zalf ontspant de spanning in de sluitspier van het anaal kanaal. Dit verbetert de doorbloeding van de anale fissuur en zodoende de genezing.
– De crème moet 2-4 keer per dag worden aangebracht. Het moet worden aangebracht in het anaal kanaal. De crème moet op de vingertop worden aangebracht (dat kan met een condoom of met een uitgeknipte vinger van een plastieken handschoen).
– De behandeling duurt meestal 4 weken. Als de symptomen snel verminderen, kan de frequentie en de duur van het aanbrengen van de crème in overleg met uw arts worden verminderd.
– Genezing van de fissuur: 40-60%.
– Bijwerkingen van de zalf: Hoofdpijn: 15-39%
Cochrane library ; Review. Operative procedures in fissura in ano ; Nov 2011
Richard Nelson British medical journal Clinical Evidence 2014;11:407
JH ScholefieldA dose finding study with 0.1%, 0.2%, and 0.4% glyceryl trinitrate ointment in patients with chronic anal fissures Gut 2003 52 (2) 264-269
A Comparison of Injections of Botulinum Toxin and Topical Nitroglycerin Ointment for. the Treatment of Chronic Anal Fissure N Engl J Med 1999; 341:65-69
Wat zijn de mogelijke chirurgische behandelingen?
De ingreep (dat zal worden aanbevolen,) wordt geval per geval bepaald, in functie van de kenmerken van de anale fissuur en de patiënt.
- Fissurectomie en Botuline toxine (Botox®) injecties
De operatie bestaat uit het verwijderen van de kloof en de open wonde te laten ophelen. Botuline toxine wordt in de inwendige sluitspier geïnjecteerd waardoor deze gedeeltelijk en tijdelijk verlamd wordt, Hierdoor zal de spanning van de anale sluitspier afnemen. De bloedvoorziening ter hoogte van de wonde zal dan toenemen , hetgeen de genezing van de wonde bevorderd.
Zie operatie: Fissurectomie en Botulinetoxine (Botox®) injecties
- Fissurectomie en laterale sphincterotomie
De operatie bestaat uit het verwijderen en de open wonde te laten ophelen. De interne sluitspier wordt gedeeltelijk ingesneden zodat de spanning van de anale sluitspier afneemt en aldus de bloedvoorziening van de wonde toeneemt en de genezing van de wonde bevorderd wordt.
Zie operatie: Fissurectomie en laterale sfincterotomie
- Fissurectomie en anoplastie
De operatie bestaat uit het wegsnijden van de fissuur en het bedekken van de wonde met gezond weefsel.