Operation
 Print this article
Print this article Download the article
Download the article Making an appointment
Making an appointmentIndication
- High transsphincteric fistula (involving more than 30% of the anal sphincter).
- Anterior fistula in a woman (internal opening of the fistula anterior in the anal front sphincter in supine position).
- In case of recurrence of an anal fistula.
- In case of pre-existing fecal incontinence.
- Anal fistula with multiple internal openings and tracts.
- Fistula after inflammatory disease, radiotherapy, tuberculosis, malignancy.
Surgery
Drainage of the fistula tract is indicated if the risk of incontinence with a fistulectomy/fistulotomy procedure is deamed to be too high.
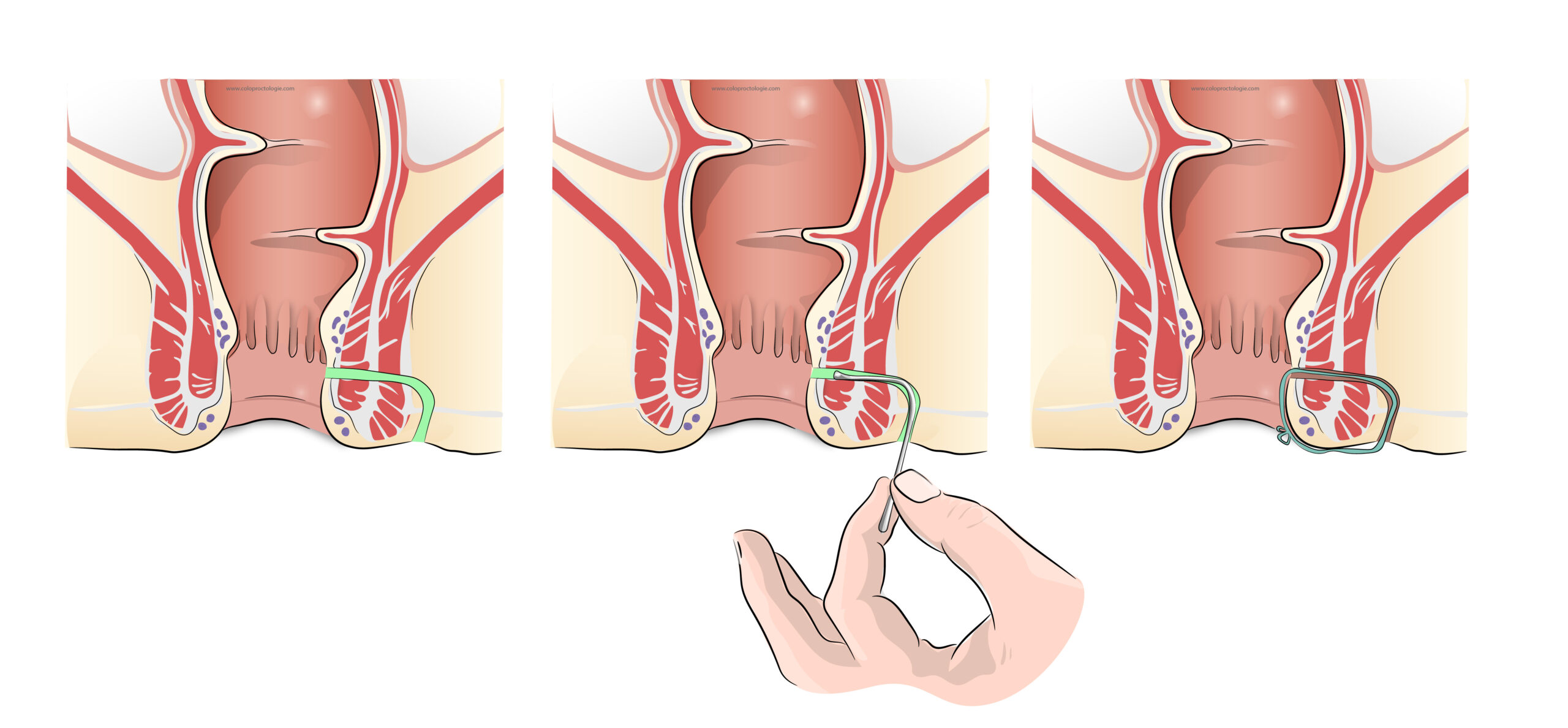
In most cases, placement of a plastic drainage wire (Seton®) is the first stage of a two-stage procedure. The second stage consists of a rectal advancement flap or an intersphincteric ligature of the fistula tract after at least 6 weeks.
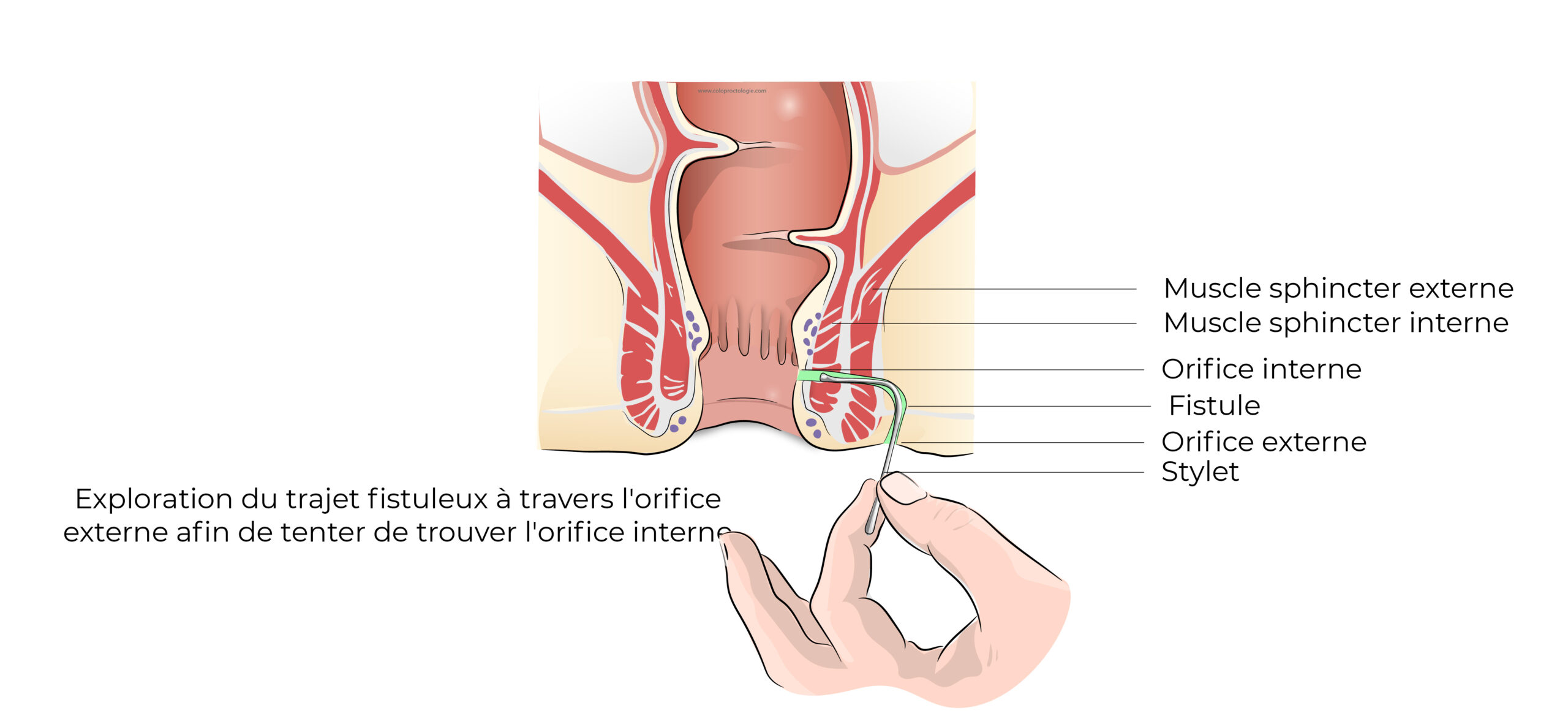
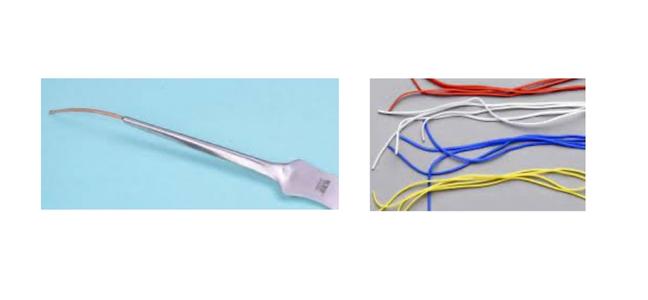
During surgery, a stylet (thin metal rod) is inserted along the external opening of the fistula and attempts are made to find the trajectory from the external to the internal opening while avoiding to create a new tract at all costs.
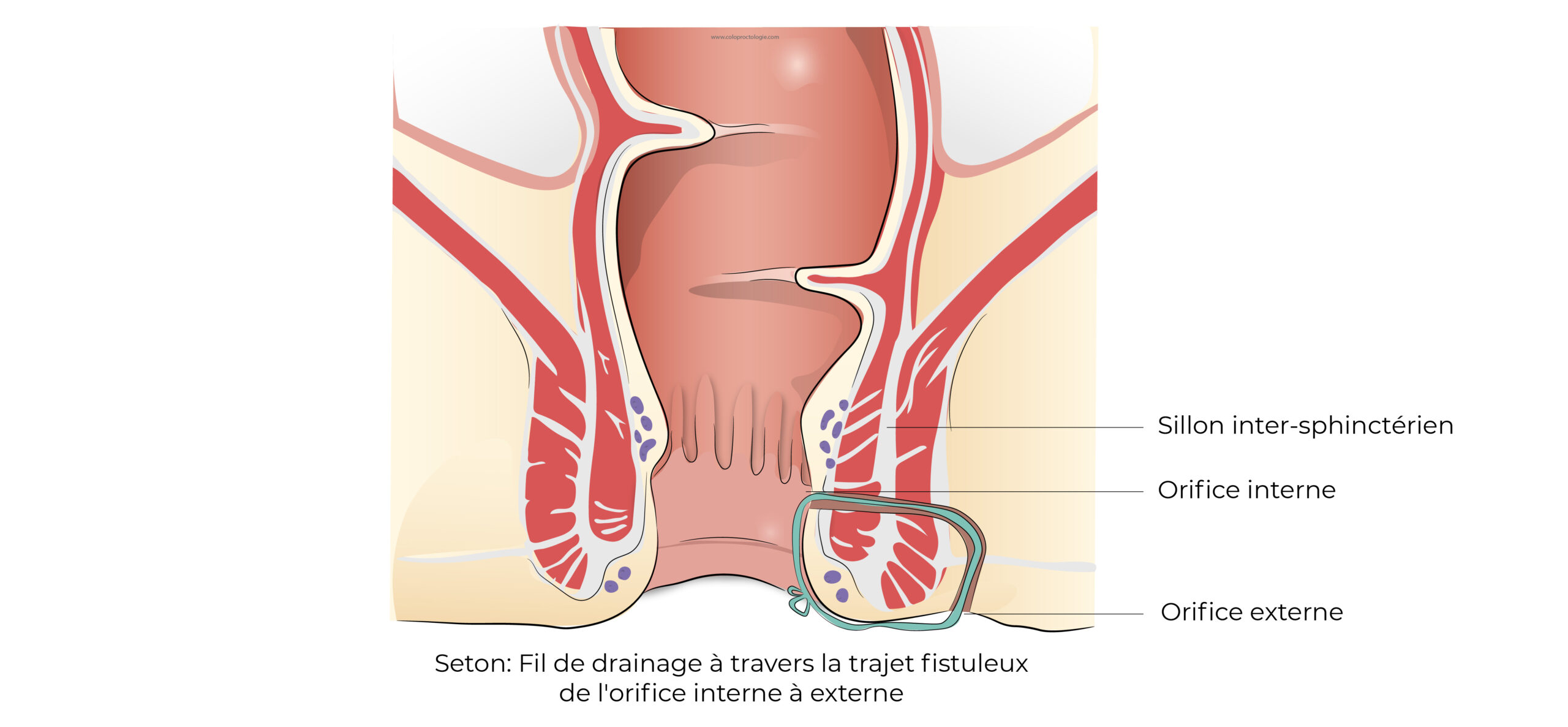
Once the tract is identified, a flexible plastic wire will be inserted through the internal and external openings along the fistula tract, after which the two ends are knotted together.
In this way, the wire drains the infection, awaiting the second stage of surgery.
In 25-30% of cases, the internal opening cannot be fined and the tract cannot be identified, subsequently no drainage wire is inserted during the procedure.
Duration of surgery :
- +/- 30 min
Wound healing :
- No wound healing
Complications
The tract and the internal opening cannot be identified
-
+/- 25 – 30%
Recurrence
-
Making a false trajectory with the stylet when looking for the internal opening. One should absolutely avoid making a new trajectory as this increases the risk of recurrence.
Break
-
Loosening/breakage of the drainage wire (Seton®).
Normal – abnormal symptoms
Normal symptoms
- Anal pain is normal but should subside over time.
- Seepage of serous (yellowish) anal fluid.
- Fluid loss may be bloody but should subside over time.
Abnormal symptoms
Contact your surgeon or GP, or go to the emergency room:
- If pain increases over time.
- If fever does not subside over time.
- If pus volume increases or foul smelling viscous fluid increases.
- If blood loss persists.
If certain symptoms seem abnormal to you contact your doctor.
If this is not possible, you can contact avec your surgeon.
If you are unable to contact your GP or your surgeon, go to the emergency department at St Elizabeth Hospital in Uccle.
Functional Results
Incontinence
There is no risk of incontinence when a plastic drainage wire (Seton®) is inserted.